

Subcutaneous infusion of high-dose benzathine penicillin G is safe, tolerable, and suitable for less-frequent dosing for rheumatic heart disease secondary prophylaxis: a phase 1 open-label population pharmacokinetic study
- PMID: 37971244
- PMCID: PMC10720493
- DOI: 10.1128/aac.00962-23
Subcutaneous infusion of high-dose benzathine penicillin G is safe, tolerable, and suitable for less-frequent dosing for rheumatic heart disease secondary prophylaxis: a phase 1 open-label population pharmacokinetic study
Abstract
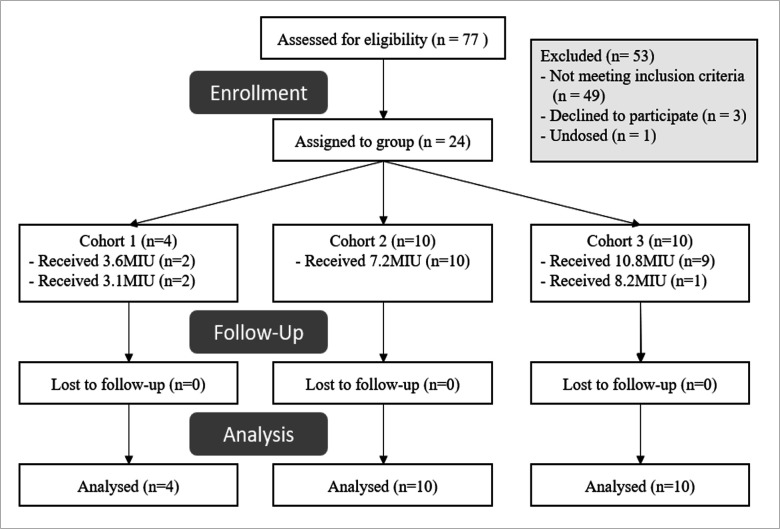
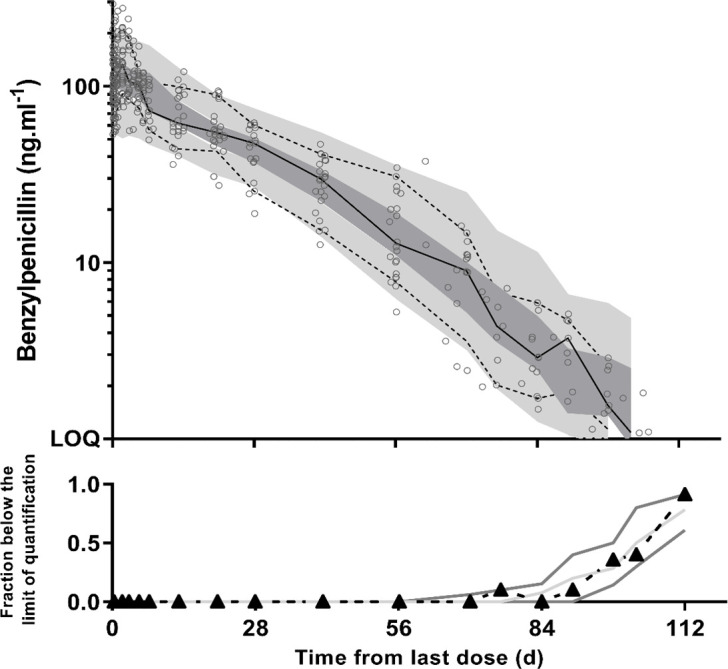
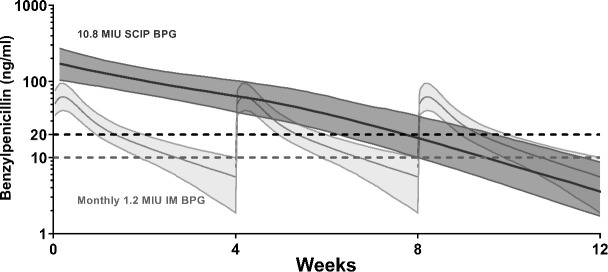
Since 1955, the recommended strategy for rheumatic heart disease (RHD) secondary prophylaxis has been benzathine penicillin G [BPG; 1.2 MU (900 mg)] injections administered intramuscularly every 4 weeks. Due to dosing frequency, pain, and programmatic challenges, adherence is suboptimal. It has previously been demonstrated that BPG delivered subcutaneously at a standard dose is safe and tolerable and has favorable pharmacokinetics, setting the scene for improved regimens with less frequent administration. The safety, tolerability, and pharmacokinetics of subcutaneous infusions of high-dose BPG were assessed in 24 healthy adult volunteers assigned to receive either 3.6, 7.2, or 10.8 MU (three, six, and nine times the standard dose, respectively) as a single subcutaneous infusion. The delivery of the BPG to the subcutaneous tissue was confirmed with ultrasonography. Safety assessments, pain scores, and penicillin concentrations were measured for 16 weeks post-dose. Subcutaneous infusion of penicillin (SCIP) was generally well tolerated with all participants experiencing transient, mild infusion-site reactions. Prolonged elevated penicillin concentrations were described using a combined zero-order (44 days) and first-order (t1/2 = 12 days) absorption pharmacokinetic model. In simulations, time above the conventionally accepted target concentration of 20 ng/mL (0.02 µg/mL) was 57 days for 10.8 MU delivered by subcutaneous infusion every 13 weeks compared with 9 days of every 4-weekly dosing interval for the standard 1.2 MU intramuscular dose (i.e., 63% and 32% of the dosing interval, respectively). High-dose SCIP (BPG) is safe, has acceptable tolerability, and may be suitable for up to 3 monthly dosing intervals for secondary prophylaxis of RHD.
Keywords: benzathine penicillin G; population pharmacokinetics; rheumatic heart disease; secondary antibiotic prophylaxis; subcutaneous infusions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
"Hurts less, lasts longer"; a qualitative study on experiences of young people receiving high-dose subcutaneous injections of benzathine penicillin G to prevent rheumatic heart disease in New Zealand.PLoS One. 2024 May 14;19(5):e0302493. doi: 10.1371/journal.pone.0302493. eCollection 2024. PLoS One. 2024. PMID: 38743745 Free PMC article. Clinical Trial.
-
Qualitative assessment of healthy volunteer experience receiving subcutaneous infusions of high-dose benzathine penicillin G (SCIP) provides insights into design of late phase clinical studies.PLoS One. 2023 Apr 27;18(4):e0285037. doi: 10.1371/journal.pone.0285037. eCollection 2023. PLoS One. 2023. PMID: 37104500 Free PMC article. Clinical Trial.
-
High dose, subcutaneous injections of benzathine penicillin G (SCIP) to prevent rheumatic fever: A single arm, phase IIa trial of safety and pharmacokinetics.J Infect. 2025 Jul;91(1):106506. doi: 10.1016/j.jinf.2025.106506. Epub 2025 May 14. J Infect. 2025. PMID: 40378963 Clinical Trial.
-
Severe adverse reactions to benzathine penicillin G in rheumatic heart disease: A systematic review and meta-analysis.PLoS One. 2025 May 7;20(5):e0322873. doi: 10.1371/journal.pone.0322873. eCollection 2025. PLoS One. 2025. PMID: 40333929 Free PMC article.
-
Are the currently recommended doses of benzathine penicillin G adequate for secondary prophylaxis of rheumatic fever?Pediatrics. 1996 Jun;97(6 Pt 2):989-91. Pediatrics. 1996. PMID: 8637788 Review.
Cited by
-
"Hurts less, lasts longer"; a qualitative study on experiences of young people receiving high-dose subcutaneous injections of benzathine penicillin G to prevent rheumatic heart disease in New Zealand.PLoS One. 2024 May 14;19(5):e0302493. doi: 10.1371/journal.pone.0302493. eCollection 2024. PLoS One. 2024. PMID: 38743745 Free PMC article. Clinical Trial.
-
Qualitative assessment of healthy volunteer experience receiving subcutaneous infusions of high-dose benzathine penicillin G (SCIP) provides insights into design of late phase clinical studies.PLoS One. 2023 Apr 27;18(4):e0285037. doi: 10.1371/journal.pone.0285037. eCollection 2023. PLoS One. 2023. PMID: 37104500 Free PMC article. Clinical Trial.
-
Local anaesthetic to reduce injection pain in patients who are prescribed intramuscular benzathine penicillin G: a systematic review and meta-analysis.EClinicalMedicine. 2024 Sep 4;76:102817. doi: 10.1016/j.eclinm.2024.102817. eCollection 2024 Oct. EClinicalMedicine. 2024. PMID: 39290636 Free PMC article.
-
From Strep Infection to a Strepitous Heart Pattern in Rheumatic Fever: A Case Report.Cureus. 2024 Nov 4;16(11):e72997. doi: 10.7759/cureus.72997. eCollection 2024 Nov. Cureus. 2024. PMID: 39634993 Free PMC article.
-
Intramuscular versus enteral penicillin prophylaxis to prevent progression of rheumatic heart disease: Study protocol for a noninferiority randomized trial (the GOALIE trial).Am Heart J. 2024 Sep;275:74-85. doi: 10.1016/j.ahj.2024.05.012. Epub 2024 May 24. Am Heart J. 2024. PMID: 38797460
References
-
- Oliver J, Bennett J, Thomas S, Zhang J, Pierse N, Moreland NJ, Williamson DA, Jack S, Baker M. 2021. Preceding group A Streptococcus skin and throat infections are individually associated with acute rheumatic fever: evidence from New Zealand. BMJ Glob Health 6:e007038. doi:10.1136/bmjgh-2021-007038 - DOI - PMC - PubMed
-
- Katzenellenbogen JM, Bond-Smith D, Seth RJ, Dempsey K, Cannon J, Stacey I, Wade V, de Klerk N, Greenland M, Sanfilippo FM, Brown A, Carapetis JR, Wyber R, Nedkoff L, Hung J, Bessarab D, Ralph AP. 2020. Contemporary incidence and prevalence of rheumatic fever and rheumatic heart disease in Australia using linked data: the case for policy change. J Am Heart Assoc 9:e016851. doi:10.1161/JAHA.120.016851 - DOI - PMC - PubMed
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. . 2020. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol 76:2982–3021. doi:10.1016/j.jacc.2020.11.010 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 7012/Cure Kids (CK)
- StrepA PhD Scholarship, Scholarship for International Research Fees/University of Western Australia (UWA)
- Post Graduate Research Scholarship (Athelstan Saw Bequest Fund)/University of Western Australia (UWA)
- Research Program Training Scholarship/University of Western Australia (UWA)
- Wesfarmers Centre of Vaccines and Infectious Diseases Top Up Scholarship/Telethon Kids Institute (TKI)
LinkOut - more resources
Full Text Sources
Research Materials
