

Combined model integrating deep learning, radiomics, and clinical data to classify lung nodules at chest CT
- PMID: 37971691
- PMCID: PMC10808169
- DOI: 10.1007/s11547-023-01730-6
Combined model integrating deep learning, radiomics, and clinical data to classify lung nodules at chest CT
Abstract
Objectives: The study aimed to develop a combined model that integrates deep learning (DL), radiomics, and clinical data to classify lung nodules into benign or malignant categories, and to further classify lung nodules into different pathological subtypes and Lung Imaging Reporting and Data System (Lung-RADS) scores.
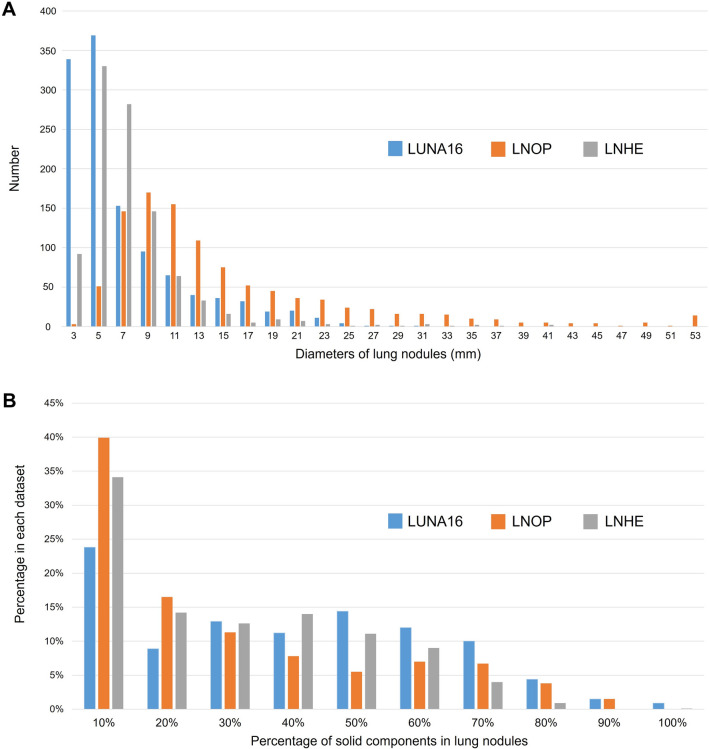
Materials and methods: The proposed model was trained, validated, and tested using three datasets: one public dataset, the Lung Nodule Analysis 2016 (LUNA16) Grand challenge dataset (n = 1004), and two private datasets, the Lung Nodule Received Operation (LNOP) dataset (n = 1027) and the Lung Nodule in Health Examination (LNHE) dataset (n = 1525). The proposed model used a stacked ensemble model by employing a machine learning (ML) approach with an AutoGluon-Tabular classifier. The input variables were modified 3D convolutional neural network (CNN) features, radiomics features, and clinical features. Three classification tasks were performed: Task 1: Classification of lung nodules into benign or malignant in the LUNA16 dataset; Task 2: Classification of lung nodules into different pathological subtypes; and Task 3: Classification of Lung-RADS score. Classification performance was determined based on accuracy, recall, precision, and F1-score. Ten-fold cross-validation was applied to each task.
Results: The proposed model achieved high accuracy in classifying lung nodules into benign or malignant categories in LUNA 16 with an accuracy of 92.8%, as well as in classifying lung nodules into different pathological subtypes with an F1-score of 75.5% and Lung-RADS scores with an F1-score of 80.4%.
Conclusion: Our proposed model provides an accurate classification of lung nodules based on the benign/malignant, different pathological subtypes, and Lung-RADS system.
Keywords: Deep learning; Lung nodule; Radiomics.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
