

Nivolumab for Patients With High-Risk Oral Leukoplakia: A Nonrandomized Controlled Trial
- PMID: 37971722
- PMCID: PMC10654930
- DOI: 10.1001/jamaoncol.2023.4853
Nivolumab for Patients With High-Risk Oral Leukoplakia: A Nonrandomized Controlled Trial
Abstract
Importance: Proliferative verrucous leukoplakia (PVL) is an aggressive oral precancerous disease characterized by a high risk of transformation to invasive oral squamous cell carcinoma (OSCC), and no therapies have been shown to affect its natural history. A recent study of the PVL immune landscape revealed a cytotoxic T-cell-rich microenvironment, providing strong rationale to investigate immune checkpoint therapy.
Objective: To determine the safety and clinical activity of anti-programmed cell death 1 protein (PD-1) therapy to treat high-risk PVL.
Design, setting, and participants: This nonrandomized, open-label, phase 2 clinical trial was conducted from January 2019 to December 2021 at a single academic medical center; median (range) follow-up was 21.1 (5.4-43.6) months. Participants were a population-based sample of patients with PVL (multifocal, contiguous, or a single lesion ≥4 cm with any degree of dysplasia).
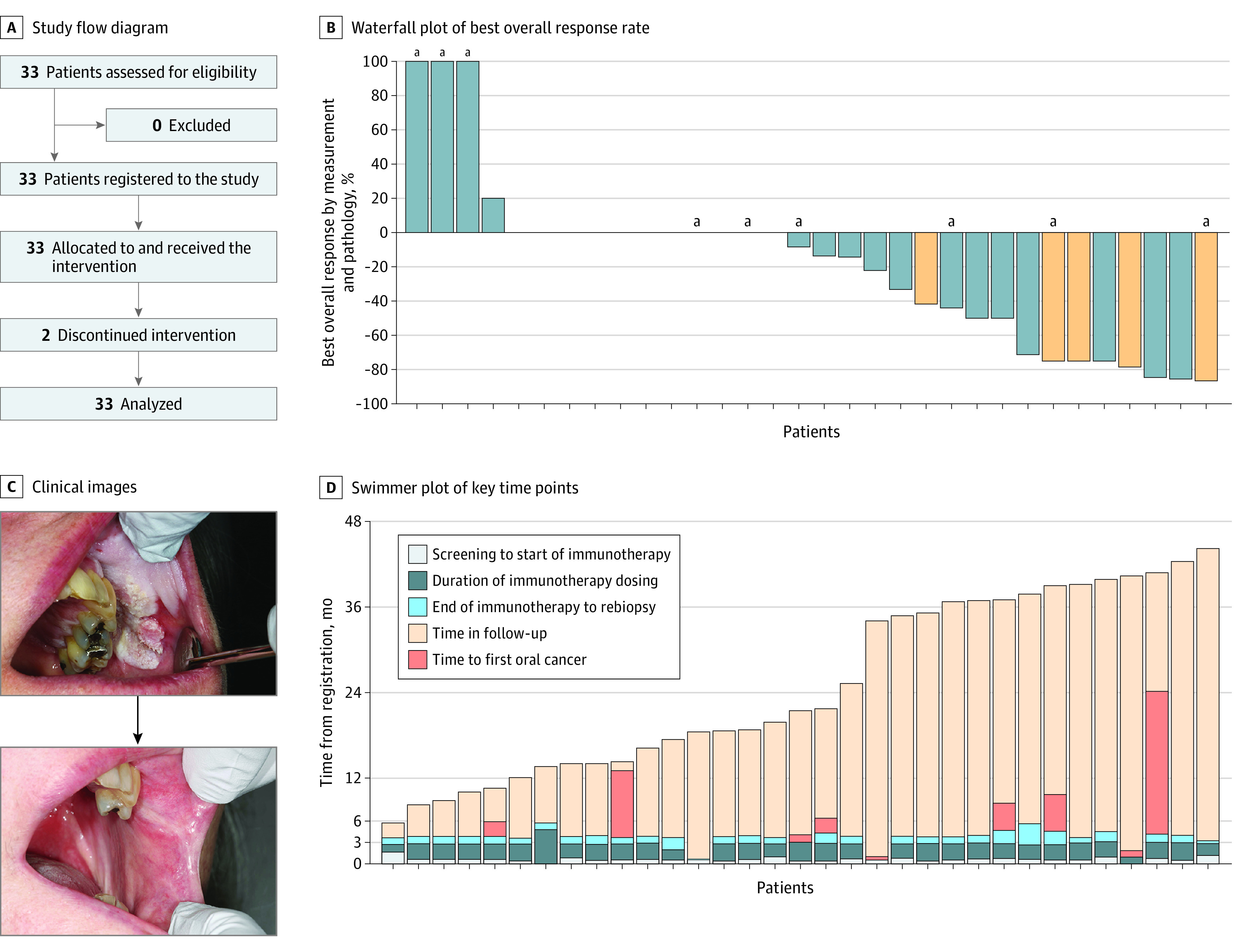
Intervention: Patients underwent pretreatment biopsy (1-3 sites) and then received 4 doses of nivolumab (480 mg intravenously) every 28 days, followed by rebiopsy and intraoral photographs at each visit.
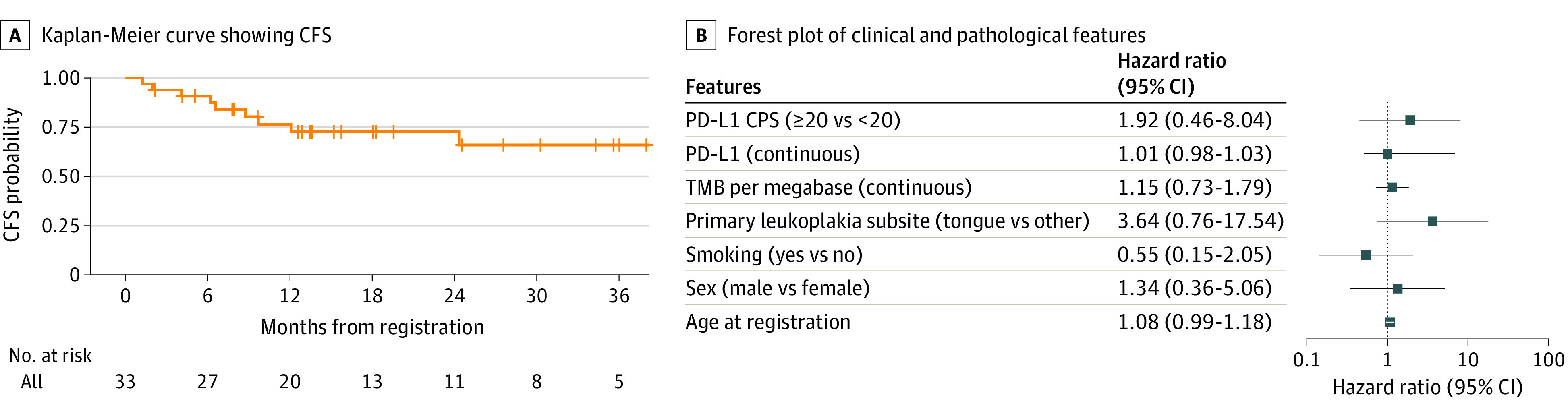
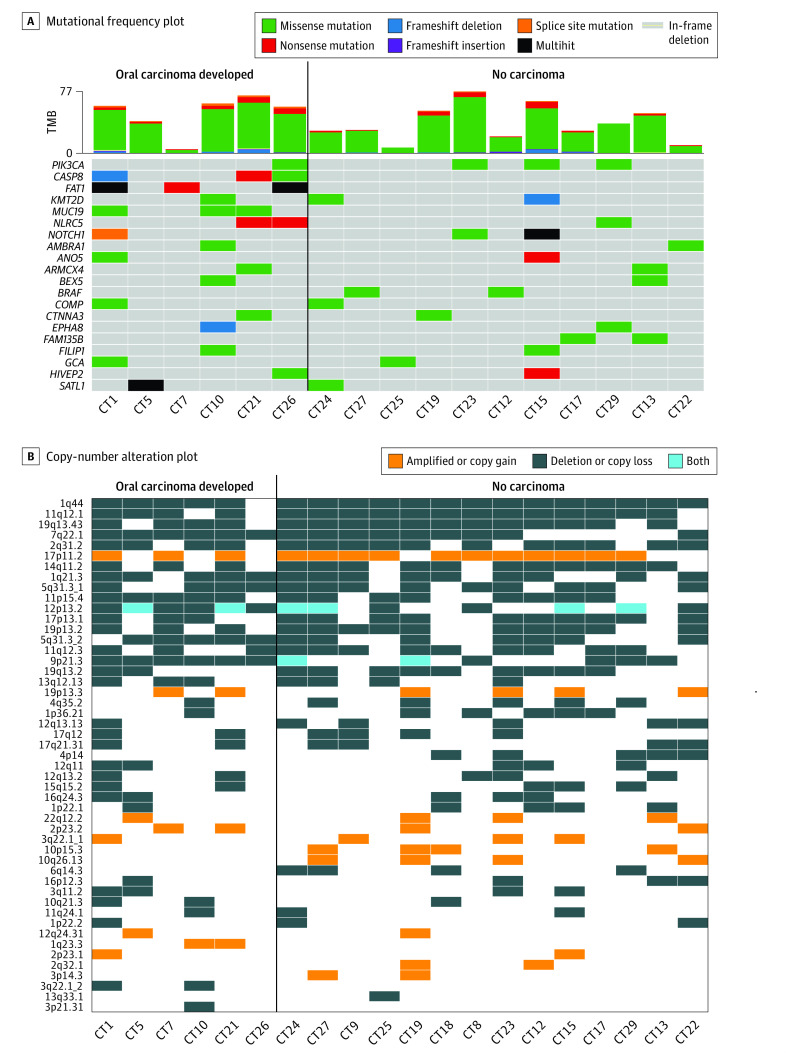
Main outcomes and measures: The primary end point was the change in composite score (size and degree of dysplasia) from before to after treatment (major response [MR]: >80% decrease in score; partial response: 40%-80% decrease). Secondary analyses included immune-related adverse events, cancer-free survival (CFS), PD-1 ligand 1 (PD-L1) expression, 9p21.3 deletion, and other exploratory immunologic and genomic associations of response.
Results: A total of 33 patients were enrolled (median [range] age, 63 [32-80] years; 18 [55%] were female), including 8 (24%) with previously resected early-stage OSCC. Twelve patients (36%) (95% CI, 20.4%-54.8%) had a response by composite score (3 MRs [9%]), 4 had progressive disease (>10% composite score increase, or cancer). Nine patients (27%) developed OSCC during the trial, with a 2-year CFS of 73% (95% CI, 53%-86%). Two patients (6%) discontinued because of toxic effects; 7 (21%) experienced grade 3 to 4 immune-related adverse events. PD-L1 combined positive scores were not associated with response or CFS. Of 20 whole-exome sequenced patients, all 6 patients who had progression to OSCC after nivolumab treatment exhibited 9p21.3 somatic copy-number loss on pretreatment biopsy, while only 4 of the 14 patients (29%) who did not develop OSCC had 9p21.3 loss.
Conclusions and relevance: This immune checkpoint therapy precancer nonrandomized clinical trial met its prespecified response end point, suggesting potential clinical activity for nivolumab in high-risk PVL. Findings identified immunogenomic associations to inform future trials in this precancerous disease with unmet medical need that has been difficult to study.
Trial registration: ClinicalTrials.gov Identifier: NCT03692325.
Conflict of interest statement
Figures
Comment in
-
Immunotherapy in Prepatients-Preventing or Promoting a Malignant Transformation?JAMA Oncol. 2024 Jan 1;10(1):41-42. doi: 10.1001/jamaoncol.2023.4799. JAMA Oncol. 2024. PMID: 37971752 No abstract available.
References
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
