

Inhaled recombinant GM-CSF reduces the need for whole lung lavage and improves gas exchange in autoimmune pulmonary alveolar proteinosis patients
- PMID: 37973175
- PMCID: PMC10764982
- DOI: 10.1183/13993003.01233-2023
Inhaled recombinant GM-CSF reduces the need for whole lung lavage and improves gas exchange in autoimmune pulmonary alveolar proteinosis patients
Abstract
Rationale: Whole lung lavage (WLL) is a widely accepted palliative treatment for autoimmune pulmonary alveolar proteinosis (aPAP) but does not correct myeloid cell dysfunction or reverse the pathological accumulation of surfactant. In contrast, inhaled recombinant granulocyte-macrophage colony-stimulating factor (rGM-CSF) is a promising pharmacological approach that restores alveolar macrophage functions including surfactant clearance. Here, we evaluate WLL followed by inhaled rGM-CSF (sargramostim) as therapy of aPAP.
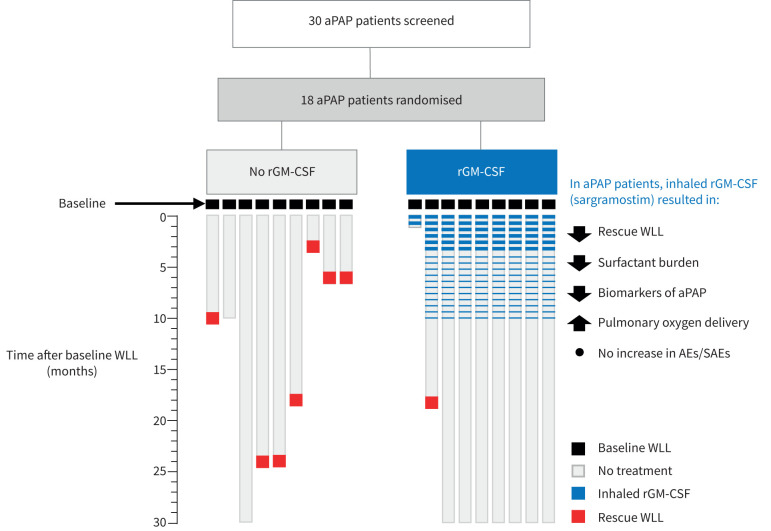
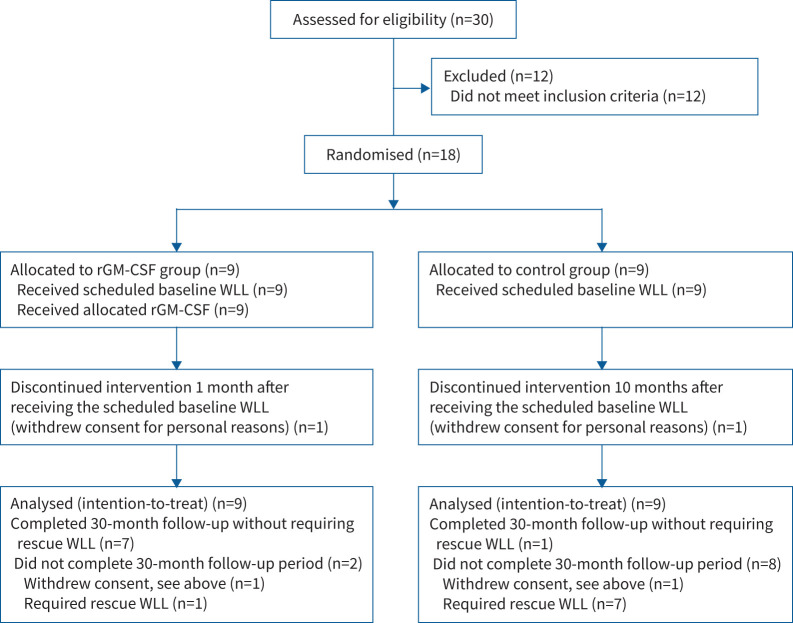
Methods: 18 patients with moderate-to-severe aPAP were enrolled, received baseline WLL, were randomised into either the rGM-CSF group (receiving inhaled sargramostim) or control group (no scheduled therapy) and followed for 30 months after the baseline WLL. Outcome measures included additional unscheduled "rescue" WLL for disease progression, assessment of arterial blood gases, pulmonary function, computed tomography, health status, biomarkers and adverse events. Patients requiring rescue WLL were considered to have failed their assigned intervention group.
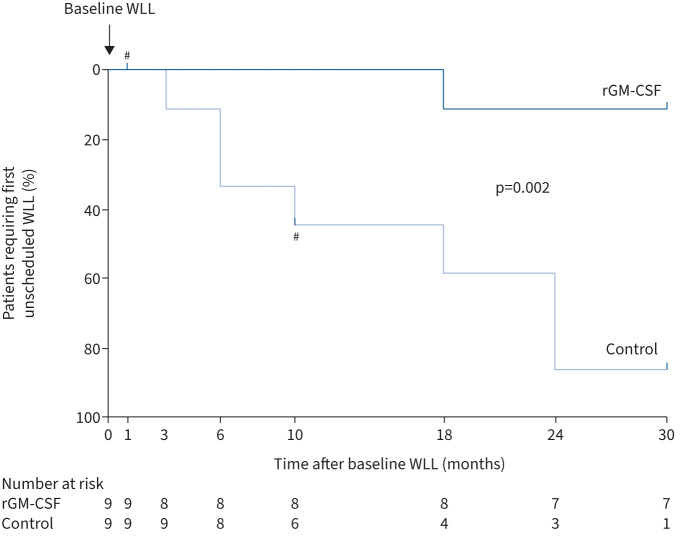
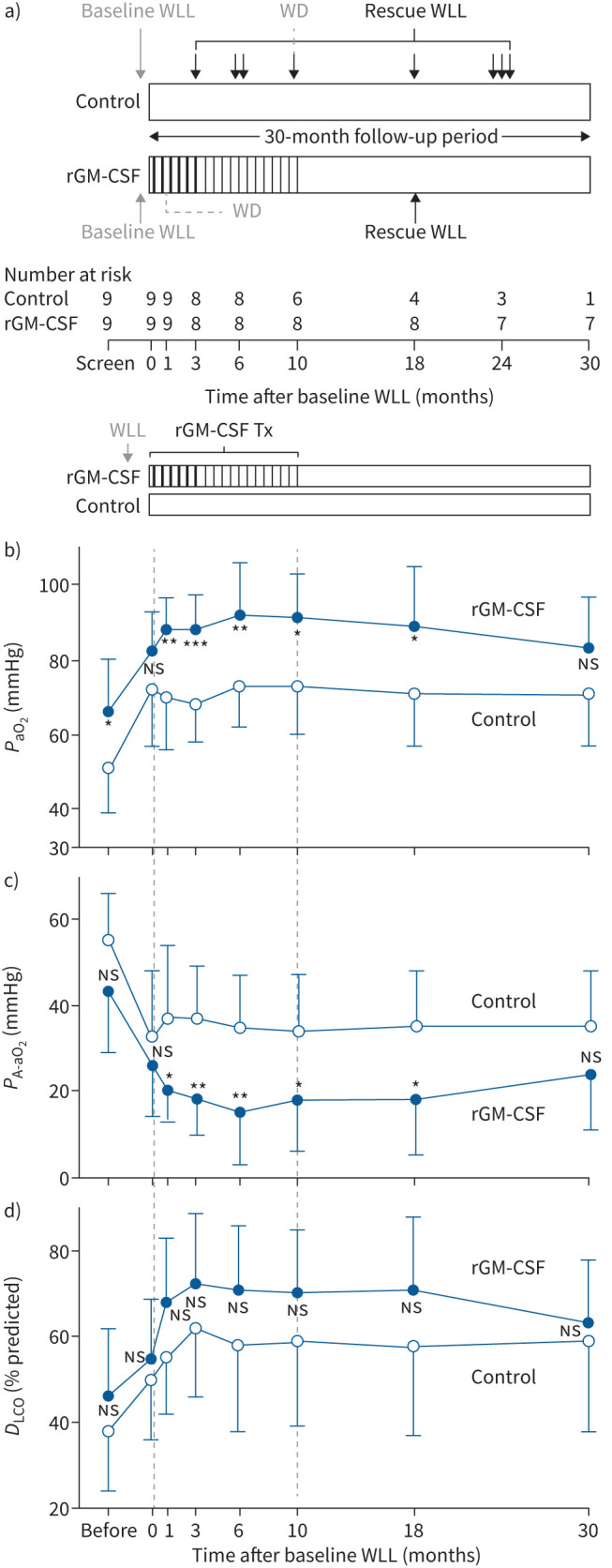
Results: The primary end-point of time to first rescue WLL was longer in rGM-CSF-treated patients than controls (30 versus 18 months, n=9 per group, p=0.0078). Seven control patients (78%) and only one rGM-CSF-treated patient (11%) required rescue WLL, demonstrating a 7-fold increase in relative risk (p=0.015). Compared to controls, rGM-CSF-treated patients also had greater improvement in peripheral arterial oxygen tension, alveolar-arterial oxygen tension difference, diffusing capacity of the lungs for carbon monoxide and aPAP biomarkers. One patient from each group withdrew for personal reasons. No serious adverse events were reported.
Conclusions: This long-term, prospective, randomised trial demonstrated inhaled sargramostim following WLL reduced the requirement for WLL, improved lung function and was safe in aPAP patients. WLL plus inhaled sargramostim may be useful as combined therapy for aPAP.
Copyright ©The authors 2024.
Conflict of interest statement
Conflict of interest: I. Campo, B.C. Trapnell and B.C. Carey serve as investigators on another clinical trial of inhaled rGM-CSF therapy of autoimmune PAP. B.C. Trapnell and B.C. Carey have served as consultants regarding the development of inhaled rGM-CSF as therapy of aPAP. No other authors have no financial or other conflicts of interest to declare related to this work.
Figures
Comment in
-
Will inhalational GM-CSF replace whole lung lavage as a treatment for autoimmune pulmonary alveolar proteinosis? Many pole positions, not yet the final winner.Eur Respir J. 2024 Jan 4;63(1):2301982. doi: 10.1183/13993003.01982-2023. Print 2024 Jan. Eur Respir J. 2024. PMID: 38176702 No abstract available.
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical