

High state boredom vastly affects psychiatric inpatients and predicts their treatment duration
- PMID: 37973905
- PMCID: PMC10654381
- DOI: 10.1038/s41398-023-02650-9
High state boredom vastly affects psychiatric inpatients and predicts their treatment duration
Abstract
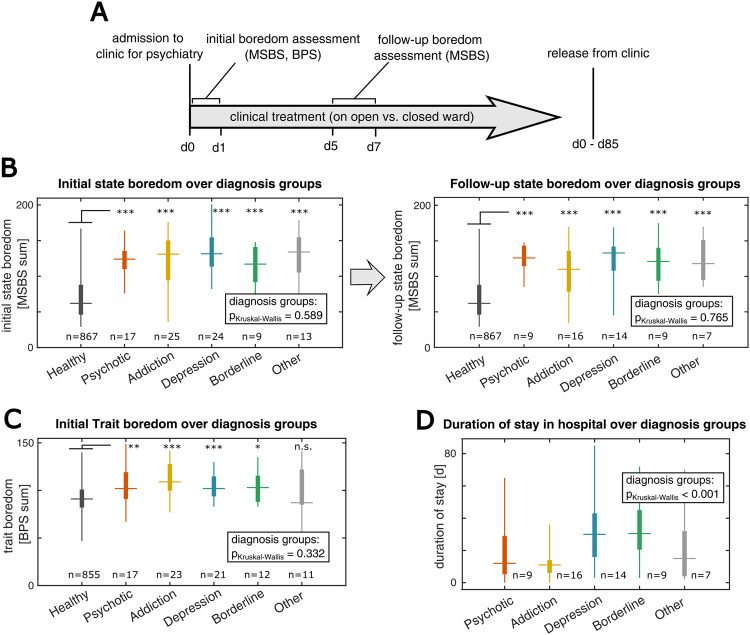
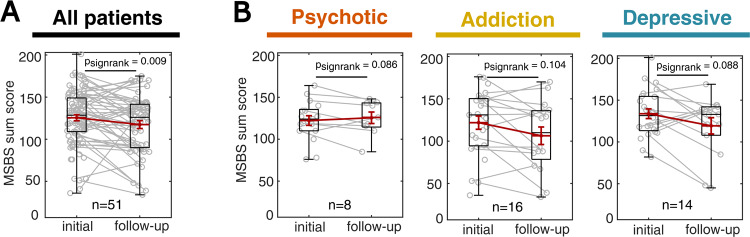
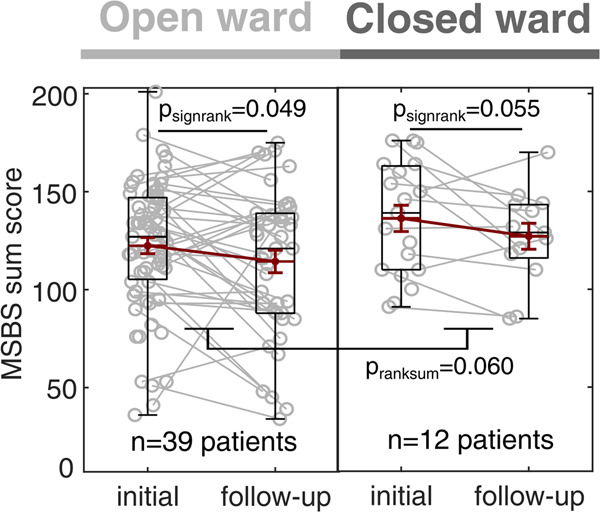
Boredom is a ubiquitous, aversive human experience typically elicited by low information and monotony. Boredom can occur either as a transient mental state that prompts individuals to adapt their behavior to avoid monotony or as a temporally stable trait, describing a chronic susceptibility to feeling bored. Increased trait boredom was found to correlate with various psychopathologies and indicators of mental burden. However, the role of state boredom in psychopathological conditions and its implications for psychiatric treatment remain elusive. Here, we address this issue by investigating state boredom and trait boredom in a cohort of psychiatric inpatients and a healthy control cohort. We find that in both groups, state boredom, even more than trait boredom, shows remarkable associations with psychopathology. In the inpatient group, state boredom is implicated broadly in multiple mental disorders and shows an association with treatment in closed psychiatric wards. Furthermore, through statistical modeling, we find that high-state boredom during inpatient therapy is predictive of a longer therapy duration. Thus, we show that state boredom constitutes an indicator of mild and severe psychopathology in different mental disorders, affecting the outcome of psychiatric patients. Potential therapeutic interventions are discussed, aiming to enhance information flow in the brain in order to alleviate boredom in clinical settings.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Elpidorou A. The bored mind is a guiding mind: toward a regulatory theory of boredom. Phenomenol Cogn Sci. 2018;17:455–84. doi: 10.1007/s11097-017-9515-1. - DOI
-
- Geana A, Wilson RC, Daw ND, Cohen JD. Boredom, information-seeking and exploration. Cogn Sci. 2016:1751–56.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
