

Risk of secondary malignancy following radiation therapy for prostate cancer
- PMID: 37973983
- PMCID: PMC10654670
- DOI: 10.1038/s41598-023-45856-z
Risk of secondary malignancy following radiation therapy for prostate cancer
Abstract
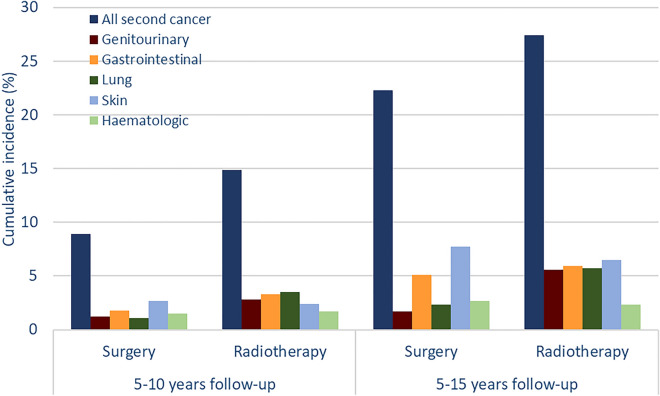
We investigated whether prostate cancer patients treated with external beam radiation therapy (EBRT) have a higher cumulative incidence of secondary cancer compared with patients treated with radical prostatectomy (RP). We used state-wide linked data from South Australia to follow men with prostate cancer diagnosed from 2002 to 2019. The cumulative incidence of overall and site-specific secondary cancers between 5 and 15 years after treatment was estimated. Fine-Gray competing risk analyses were performed with additional sensitivity analyses to test different scenarios. A total of 7625 patients were included (54% underwent RP and 46% EBRT). Characteristics of the two groups differed significantly, with the EBRT group being older (71 vs. 64 years), having higher comorbidity burden and being more likely to die during follow-up than the RP group. Fifteen-year cumulative incidence for all secondary cancers was 27.4% and 22.3% in EBRT and RP groups, respectively. In the adjusted models, patients in the EBRT group had a significantly higher risk of genitourinary (adjusted subhazard ratio (aSHR), 2.29; 95%CI 1.16-4.51) and lung (aSHR, 1.93; 95%CI 1.05-3.56) cancers compared with patients in the RP group. However, there was no statistically significant difference between the two groups for risk of any secondary cancer, gastro-intestinal, skin or haematologic cancers. No statistically significant differences in overall risk of secondary cancer were observed in any of the sensitivity analyses and patterns for risk at specific cancer sites were relatively consistent across different age restriction and latency/time-lag scenarios. In conclusion, the increased risk of genitourinary and lung cancers among men undergoing EBRT may relate partly to treatment effects and partly to unmeasured residual confounding.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Moschini M, Zaffuto E, Karakiewicz PI, Andrea DD, Foerster B, Abufaraj M, et al. External Beam radiotherapy increases the risk of bladder cancer when compared with radical prostatectomy in patients affected by prostate cancer: A population-based analysis. Eur. Urol. 2019;75(2):319–328. doi: 10.1016/j.eururo.2018.09.034. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
