

Impact of vaccination and variants of concern on long COVID clinical phenotypes
- PMID: 37974068
- PMCID: PMC10655269
- DOI: 10.1186/s12879-023-08783-y
Impact of vaccination and variants of concern on long COVID clinical phenotypes
Abstract
Background: Defining patterns of symptoms in long COVID is necessary to advance therapies for this heterogeneous condition. Here we aimed to describe clusters of symptoms in individuals with long COVID and explore the impact of the emergence of variants of concern (VOCs) and vaccination on these clusters.
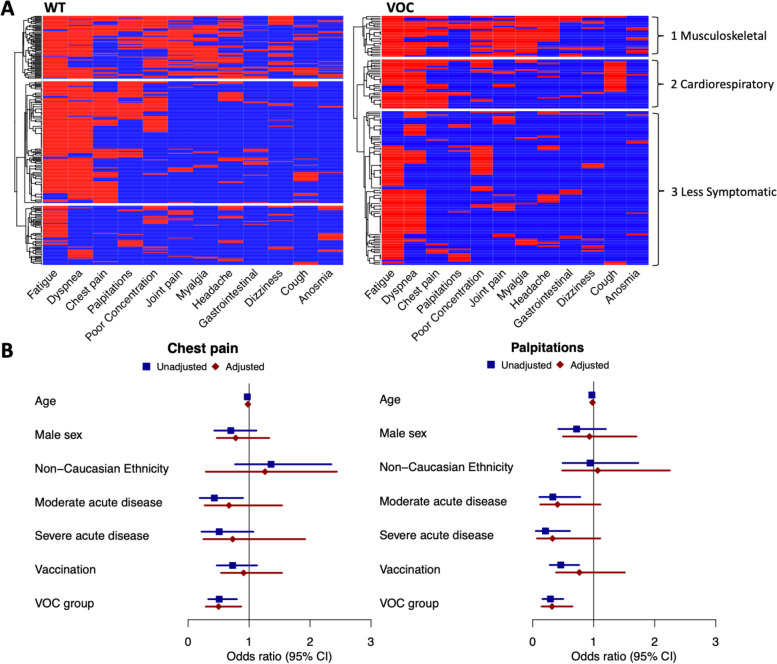
Methods: In a prospective, multi centre cohort study, individuals with symptoms persisting > 4 weeks from acute COVID-19 were divided into two groups based on timing of acute infection; pre-Alpha VOC, denoted wild type (WT) group and post-Alpha VOC (incorporating alpha and delta dominant periods) denoted VOC group. We used multiple correspondence analysis (MCA) and hierarchical clustering in the WT and VOC groups to identify symptom clusters. We then used logistic regression to explore factors associated with individual symptoms.
Results: A total of 417 individuals were included in the analysis, 268 in WT and 149 in VOC groups respectively. In both groups MCA identified three similar clusters; a musculoskeletal (MSK) cluster characterised by joint pain and myalgia, a cardiorespiratory cluster and a less symptomatic cluster. Differences in characteristic symptoms were only seen in the cardiorespiratory cluster where a decrease in the frequency of palpitations (10% vs 34% p = 0.008) and an increase in cough (63% vs 17% p < 0.001) in the VOC compared to WT groups was observed. Analysis of the frequency of individual symptoms showed significantly lower frequency of both chest pain (25% vs 39% p = 0.004) and palpitations (12% vs 32% p < 0.001) in the VOC group compared to the WT group. In adjusted analysis being in the VOC group was significantly associated with a lower odds of both chest pain and palpitations, but vaccination was not associated with these symptoms.
Conclusion: This study suggests changes in long COVID phenotype in individuals infected later in the pandemic, with less palpitations and chest pain reported. Adjusted analyses suggest that these effects are mediated through introduction of variants rather than an effect from vaccination.
Keywords: Long COVID; Post-Acute Sequelae of SARS-CoV-2 infection; SARS-CoV-2 variants.
© 2023. The Author(s).
Conflict of interest statement
E. F. has received consulting fees from Gilead, ViiV, and Vidacare Ireland, and has been awarded a grant from Science Foundation Ireland, outside the submitted work. E. D. B. has received consulting fees from Sanofi Pasteur and honoraria/travel grant from Pfizer. P. W. G. M. has received honoraria and/or travel grants from Gilead Sciences, MSD, Bristol-Myers Squibb, and ViiV Healthcare, and has been awarded grants by Science Foundation Ireland, outside the submitted work. All other authors report no potential conflicts of interest.
Figures
References
-
- Canas LS, Molteni E, Deng J, et al. Profiling post-COVID syndrome across different variants of SARS-CoV-2. MedRxiv. 2022 doi: 10.1101/2022.07.28.22278159. - DOI
-
- Zhang H, Zang C, Xu Z, et al. Machine learning for identifying Data-Driven subphenotypes of Incident Post-acute SARS-CoV-2 Infection conditions with Large Scale Electronic Health Records: findings from the RECOVER Initiative. Public Global Health. 2022. 10.1101/2022.05.21.22275412.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
