

Neurodevelopmental status and adaptive behavior of pediatric patients with mucopolysaccharidosis II: a longitudinal observational study
- PMID: 37974184
- PMCID: PMC10652632
- DOI: 10.1186/s13023-023-02805-3
Neurodevelopmental status and adaptive behavior of pediatric patients with mucopolysaccharidosis II: a longitudinal observational study
Abstract
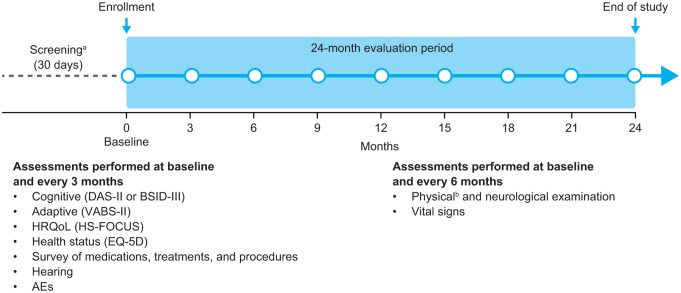
Background: Mucopolysaccharidosis (MPS) II is a rare, X-linked lysosomal storage disease. Approximately two-thirds of patients have central nervous system involvement with some demonstrating progressive cognitive impairment (neuronopathic disease). The natural history of cognitive and adaptive function in patients with MPS II is not well-defined. This 2-year, prospective, observational study evaluated the neurodevelopmental trajectories of boys with MPS II aged ≥ 2 years and < 18 years.
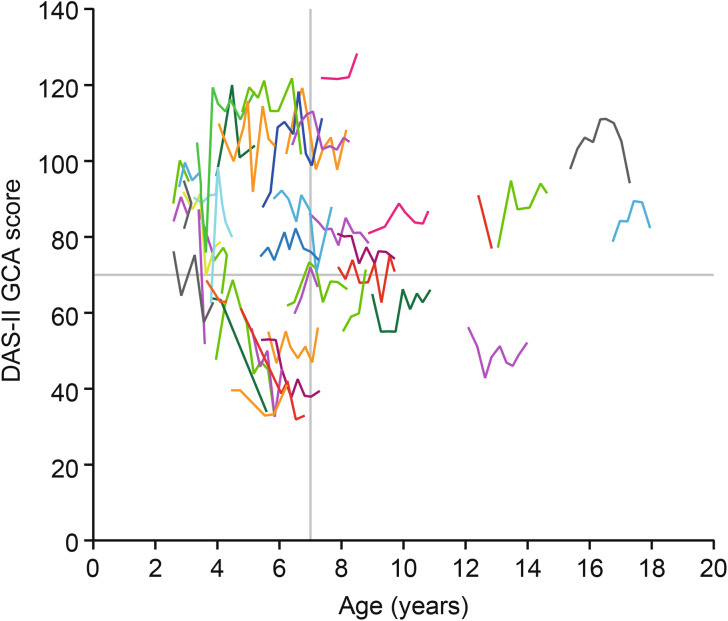
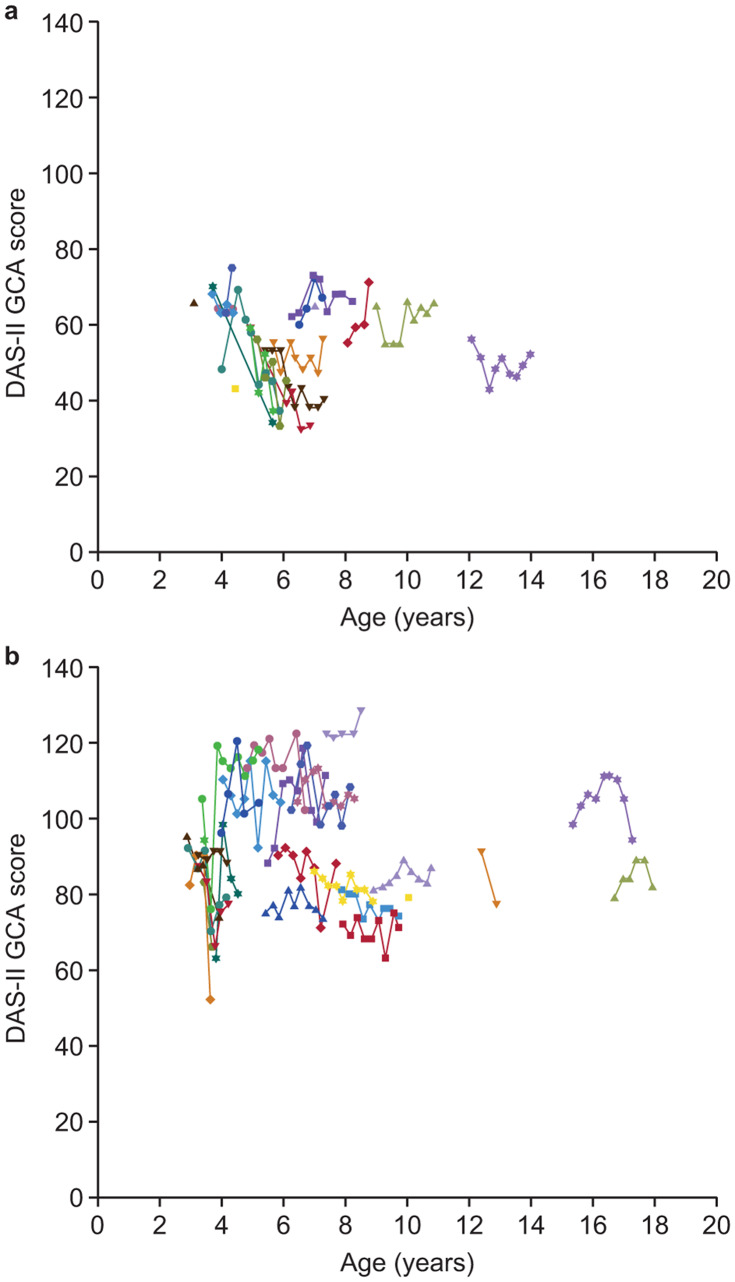
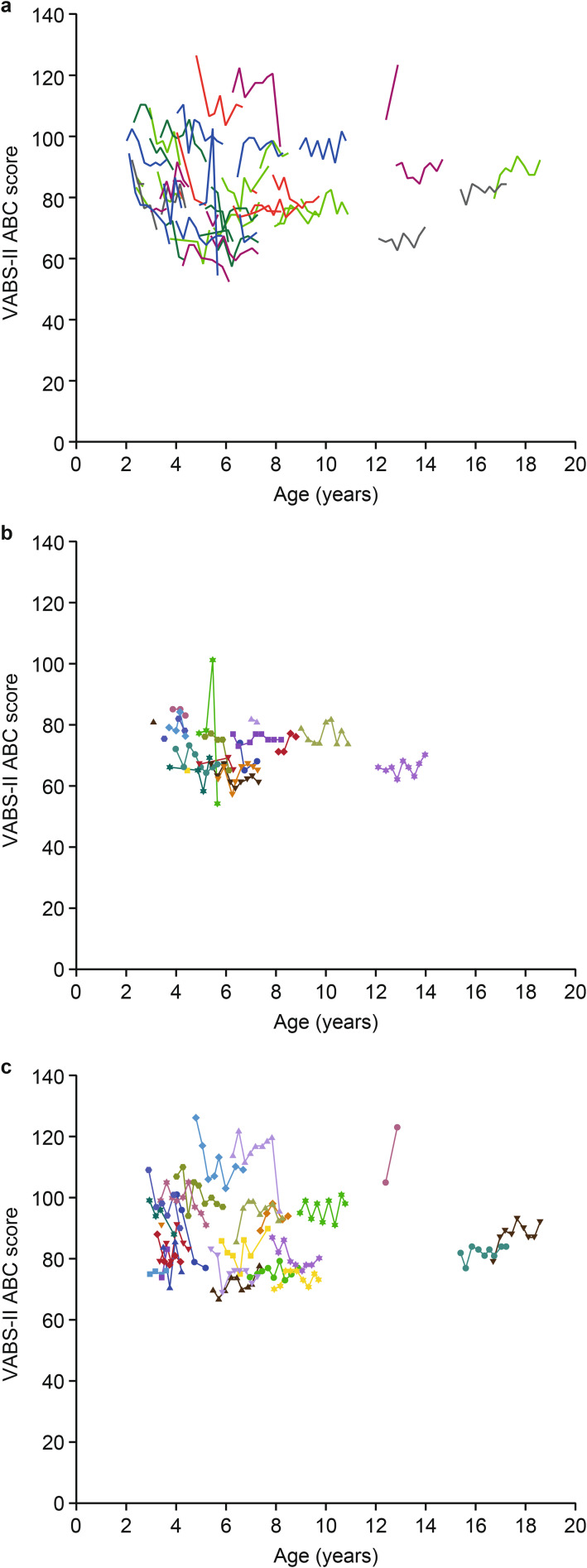
Results: Overall, 55 patients were enrolled. At baseline, mean (standard deviation [SD]) age was 5.60 (3.32) years; all patients were receiving intravenous idursulfase. Cognitive and adaptive function were assessed using the Differential Ability Scales, Second Edition (DAS-II) General Conceptual Ability (GCA) and the Vineland Adaptive Behavior Scales, Second Edition (VABS-II) Adaptive Behavior Composite (ABC) scores, respectively. Baseline mean (SD) DAS-II GCA and VABS-II ABC scores were 78.4 (19.11) and 83.7 (14.22), respectively, indicating low cognitive function and moderately low adaptive behavior. Over 24 months, modest deteriorations in mean (SD) scores were observed for DAS-II GCA (-3.8 [12.7]) and VABS-II ABC (-2.0 [8.07]). Changes in DAS-II GCA scores varied considerably, and data suggested the existence of four potential patient subgroups: (1) patients with marked early impairment and rapid subsequent decline, (2) patients with marked early impairment then stabilization, (3) patients with mild early impairment then stabilization, and (4) patients without impairment who remained stable. Subgroup analyses revealed numerically greater DAS-II GCA score reductions from baseline in patients aged < 7 years at baseline (vs. those aged ≥ 7 years) and in patients with DAS-II GCA scores ≤ 70 at baseline (vs. those with scores > 70); between-group differences were nonsignificant. No clear subgroups or patterns were identified for individual changes in VABS-II ABC scores. In total, 49 patients (89.1%) reported ≥ 1 adverse event (AE) and nine patients (16.4%) reported serious AEs.
Conclusions: Some patients with MPS II had rapid declines in cognitive ability, whereas others remained relatively stable after an initial decline. These insights provide a basis for more detailed analyses of different patient subgroups, which may enhance the definition and understanding of factors that influence cognitive and adaptive function in MPS II.
Trial registration: ClinicalTrials.gov, NCT01822184. Registered retrospectively: April 2, 2013.
Keywords: Adaptive; Behavior; Cognitive; Decline; Function; Impairment; Mucopolysaccharidosis II; Neurodevelopment; Observational; Pediatric.
© 2023. The Author(s).
Conflict of interest statement
JM has received consulting fees/other remuneration from Denali Therapeutics, JCR Pharmaceuticals, REGENXBIO, Sangamo Therapeutics, Sanofi Genzyme, and Takeda; has participated in advisory boards for BioMarin Pharmaceutical, Denali Therapeutics, JCR Pharmaceuticals, Sanofi Genzyme, and Takeda; and has received research support from BioMarin Pharmaceutical, Denali Therapeutics, and Takeda.
BKB has received consulting fees/other remuneration from Alexion Pharmaceuticals, Applied Therapeutics, BioMarin Pharmaceutical, Capsida Biotherapeutics, Denali Therapeutics, Horizon Therapeutics, JCR Pharmaceuticals, Moderna, Passage Bio, Sanofi Genzyme, Sio Gene Therapies, Takeda, and Ultragenyx Pharmaceutical; has participated in advisory boards or similar committees for Alexion Pharmaceuticals, BioMarin Pharmaceutical, and Takeda; and has received research support from Alexion Pharmaceuticals, BioMarin Pharmaceutical, Denali Therapeutics, Homology Medicines, JCR Pharmaceuticals, Sangamo Therapeutics, Takeda, and Ultragenyx Pharmaceutical.
HMA has participated in advisory boards for Takeda; has received consulting fees from BioMarin Pharmaceutical and Takeda; has been involved in contracted research for Amicus Therapeutics, Bluebird bio, and Takeda; has received fees from Amicus Therapeutics, BioMarin Pharmaceutical, Sanofi Genzyme, and Takeda; and has received other remuneration from Amicus Therapeutics, Bluebird bio, and Takeda.
PRH has received consulting fees/other remuneration from Aeglea, Alexion Pharmaceuticals, ArmaGen, Audentes, AVROBIO, BioMarin Pharmaceutical, Capsida Biotherapeutics, Chiesi, Denali Therapeutics, Edigene, Enzyvant, Fondazione Telethon, Grace Science, Inventiva Pharma, JCR Pharmaceuticals, Novel Pharma, Orchard Therapeutics, Orphazyme, Paradigm Biopharma, PTC Therapeutics, Rallybio, REGENXBIO, Renoviron, Saliogen, Sangamo Therapeutics, Sanofi Genzyme, Takeda, and Ultragenyx Pharmaceutical; and has received research support from Adrenas Therapeutics, Amicus Therapeutics, Alexion Pharmaceuticals, ArmaGen, Ascendis Pharma, Aspa Therapeutics, Azafaros, BioMarin Pharmaceutical, Calcilytix, Denali Therapeutics, Enzyvant, Homology Medicines, Inventiva Pharma, JCR Pharmaceuticals, Orphazyme, Prevail Therapeutics, REGENXBIO, Sangamo Therapeutics, Swedish Orphan Biovitrum, Takeda, and Ultragenyx Pharmaceutical.
LGG-S has received consulting fees/other remuneration from BioMarin Pharmaceutical, Sanofi Genzyme, Takeda, and Ultragenyx Pharmaceutical; and has received research support from Takeda.
MR-G has received consulting fees/other remuneration and research support from Takeda.
YW is an employee of Takeda Development Center Americas, Inc. and is a stockholder of Takeda Pharmaceuticals Company Limited.
DM is an employee of Takeda Development Center Americas, Inc. and is a stockholder of Takeda Pharmaceuticals Company Limited.
DA was an employee of Takeda Development Center Americas, Inc. at the time of this study and of the writing of the manuscript (now with Merck) and is a stockholder of Takeda Pharmaceuticals Company Limited.
SAJ has received consulting fees/other remuneration from Alexion Pharmaceuticals, AVROBIO, BioMarin Pharmaceutical, Denali Therapeutics, Orchard Therapeutics, REGENXBIO, Sanofi Genzyme, Takeda, and Ultragenyx Pharmaceutical; and has received research support from Avrobio, Orchard Therapeutics, and Takeda.
Figures
References
-
- Neufeld E, Muenzer J. The mucopolysaccharidoses. In: Scriver C, Beaudet A, Sly W, Valle D, editors. The metabolic and molecular bases of inherited disease. New York: McGraw-Hill; 2001. pp. 3421–52.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
