

Adenoidectomy: Anatomical Versus Clinical Success
- PMID: 37974787
- PMCID: PMC10645738
- DOI: 10.1007/s12070-023-03992-y
Adenoidectomy: Anatomical Versus Clinical Success
Abstract
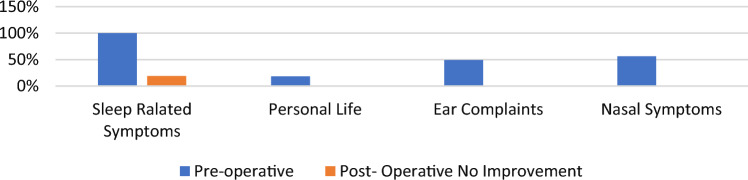
Endoscopic adenoidectomy with powered instruments,a challenge in resource-constraint developing countries, has been on the rise. To evaluate conventional curettage as compared to endoscopic assisted adenoidectomy in the successful management of adenoid enlargement. A randomized controlled double-blinded study among children undergoing adenoidectomywas done. Primary outcomes were assessed by pre- and postoperative evaluation with a symptoms questionnaire and fiberoptic nasal endoscopy. There were 71 children aged 3-15 years, majority having grade III adenoids. Conventional adenoidectomy was done by the surgeon who was blinded to preoperative adenoid status. Patients were randomized to two groups, 35in conventional curettage where no further on-table intervention was done. Check endoscopyof the remaining 36 patients, formingthe second group, revealed residual grade III adenoidsin 5.6%. They underwentcompletion adenoidectomyendoscopically. By the 12th postoperative week, nasal endoscopy noted that 39.3% had grade I/II and 8.8% had grade I in the conventional and endoscopic groups respectively. Thoughstatistically significant, all pre-op symptoms settled except sleep-related ones which persisted in both groups (25% versus 14.7) with no complications in either group. Relief of all symptoms other than sleep-related ones, was achieved despite residual adenoids being up to grade II in both conventional and endoscopic group. This suggests non-obstructive causes in a subset of these patients. Conventional adenoid curettage is comparable to endoscopic adenoidectomy by cold method among children aged three and above. Complete adenoidclearance for achieving 'anatomical success' appears not to be necessary for 'clinical success'.
Keywords: Anatomical and clinical success; Conventional adenoidectomy; Endoscopic adenoidectomy.
© Association of Otolaryngologists of India 2023. Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of interestNone.
Figures

References
-
- Robb PJ. The adenoid and adenoidectomy. In: Watkinson J, Clarke R, editors. Scott-Brown's otorhinolaryngology and head and neck surgery. 8. Boca Raton: CRC Press; 2019. pp. 285–2904.
-
- Lee CH, Hsu WC, Ko JY, Yeh TH, Lin MT, Kang KT. Revision adenoidectomy in children: a meta-analysis. Rhinology. 2019;57(6):411–419. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous