

My 40-Year Encounter with ERCP: A Saga of Service, Syndromes, and Solutions
- PMID: 37975034
- PMCID: PMC10643499
- DOI: 10.1016/j.jceh.2023.05.010
My 40-Year Encounter with ERCP: A Saga of Service, Syndromes, and Solutions
Abstract
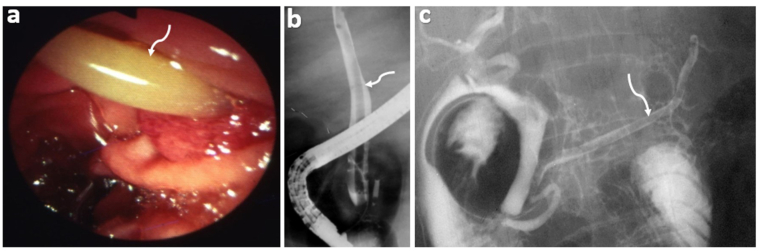
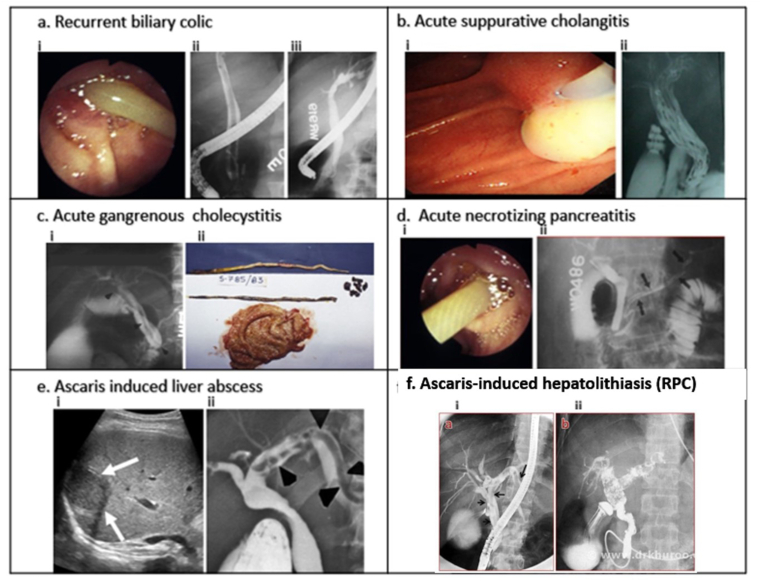
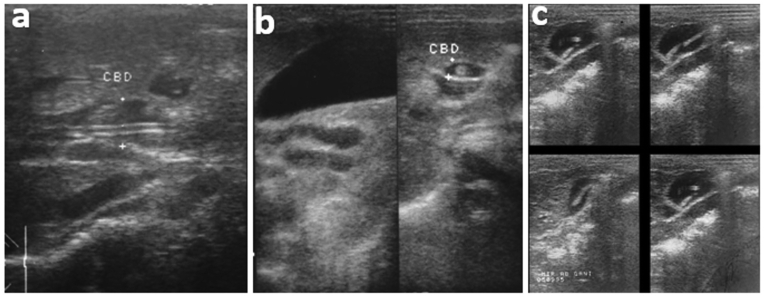
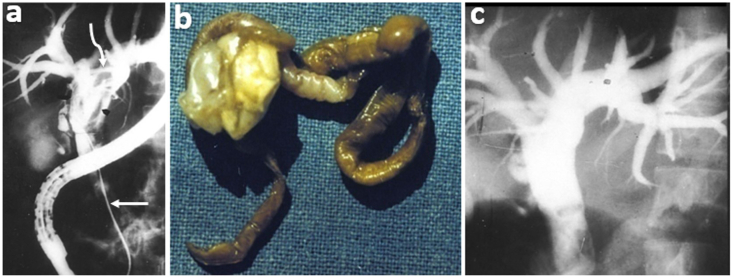
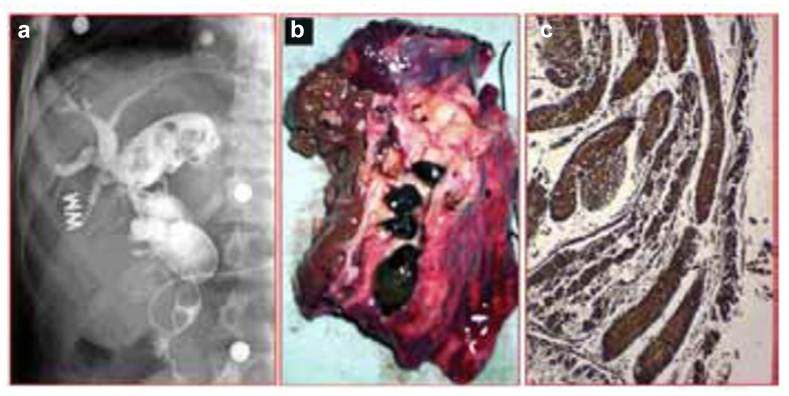
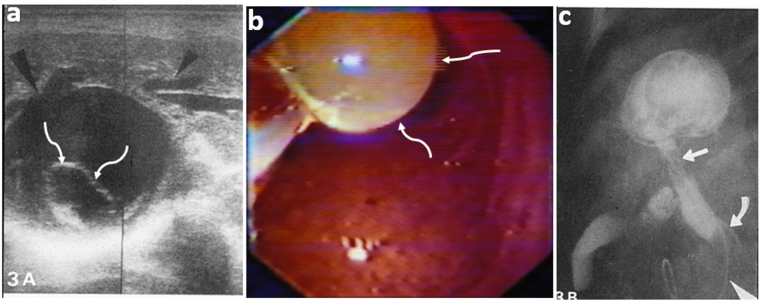
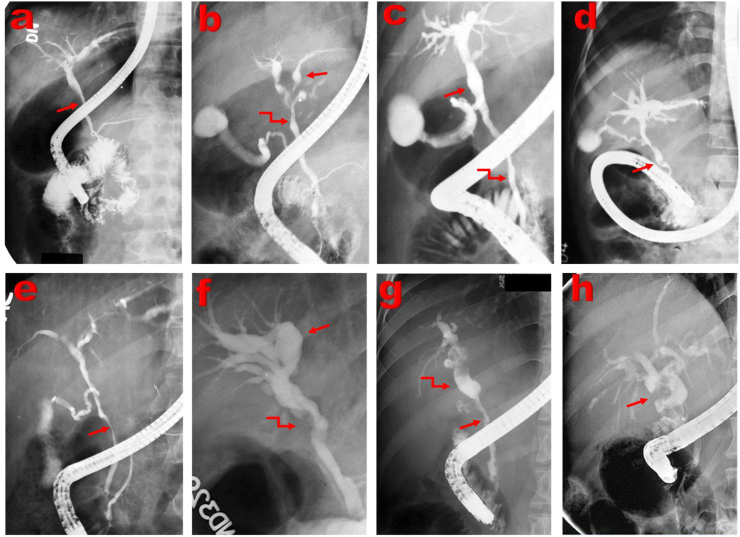
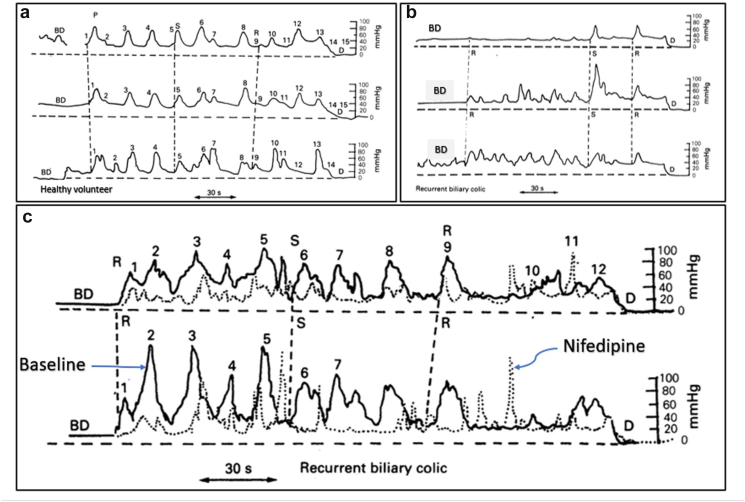
Endoscopic retrograde cholangiopancreatography (ERCP) has been a significant development in gastrointestinal endoscopy. I did my first ERCP at SKIMS on December 5, 1982, and over the last 40 years, I have performed 10,100 ERCP procedures, including 600 Sphincter of Oddi manometries (SOM), and 3200 therapeutic ERCPs. We were confronted with many clinical challenges that needed answers by applying ERCP as a primary diagnostic tool. These studies gave birth to and/or recognition of several clinical syndromes. The hepatobiliary and pancreatic ascariasis (HBPA) as a clinical disease was recognized in 1985. The nematode, Ascaris lumbricoides, was the most common cause of hepatobiliary and pancreatic diseases in Kashmir, and its impact on healthcare, clinical profile, management policies, and control measures was identified. Kashmir was recognized as an endemic zone for recurrent pyogenic cholangitis (RPC), which constituted 12.5% of all biliary diseases. RPC in this population was found essentially to be an aftermath of HBPA. A subset of patients with hepatic hydatidosis with rupture into the biliary tract was recognized at ERCP and primarily treated by endotherapy. Cholangiographic abnormalities in children with portal cavernoma evolved into the recognition of portal biliopathy. Extensive studies of the sphincter of Oddi manometry in patients with unexplained biliary and/or pancreatic pain following cholecystectomy identified the entity of the sphincter of Oddi dyskinesia (SOD). In a cross-over trial, Nifedipine, compared with a placebo, showed a significant clinical response in 20 of 28 such patients. ERCP studies done in patients with tropical calcific pancreatitis showed an anomalous union of bile and pancreatic ducts. Forty of the 220 patients with liver transplantation had biliary complications namely biliary leaks, bile duct strictures, SOD, and recurrence of underlying primary biliary cholangitis. Biliary complications caused considerable morbidity and mortality in patients with liver transplantation.
Keywords: ERCP; Portal biliopathy; ascariasis; recurrent pyogenic cholangitis; sphincter of Oddi dyskinesia.
© 2023 Indian National Association for Study of the Liver. Published by Elsevier B.V. All rights reserved.
Figures

References
-
- Oi I., Kobayashi S., Kondo T. Endoscopic pancreatocholangiography. Endoscopy. 1970;2:103–106.
-
- Ogoshi K., Tobita Y., Hara Y. Endoscopic observation of the duodenum and pancreatocholedochography, using duodenal fibrescope under direct vision. Gastroent Endosc (Tokyo) 1970;12:83–86. (Translation)
Publication types
LinkOut - more resources
Full Text Sources
