

Efficacy of four anti-vascular endothelial growth factor agents and laser treatment for retinopathy of prematurity: A network meta-analysis
- PMID: 37976345
- PMCID: PMC11293245
- DOI: 10.17305/bb.2023.9829
Efficacy of four anti-vascular endothelial growth factor agents and laser treatment for retinopathy of prematurity: A network meta-analysis
Abstract
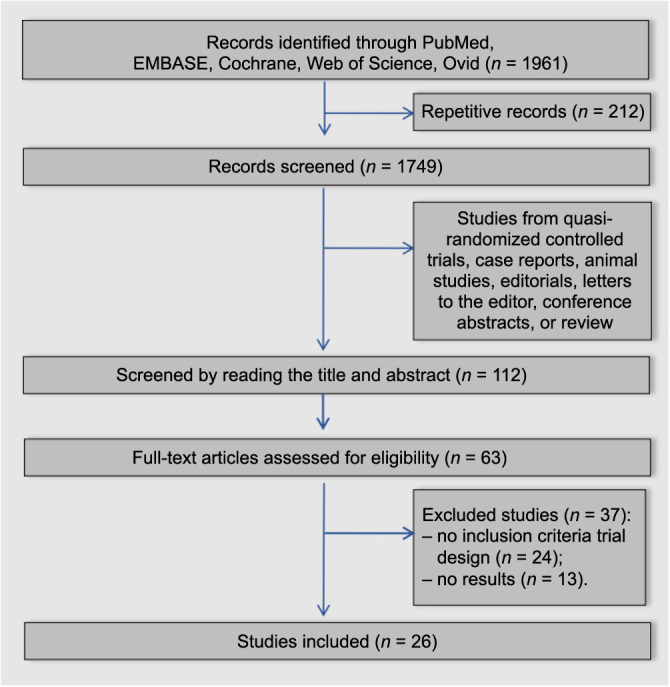
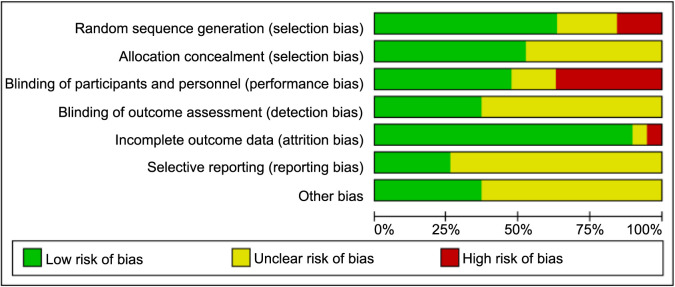
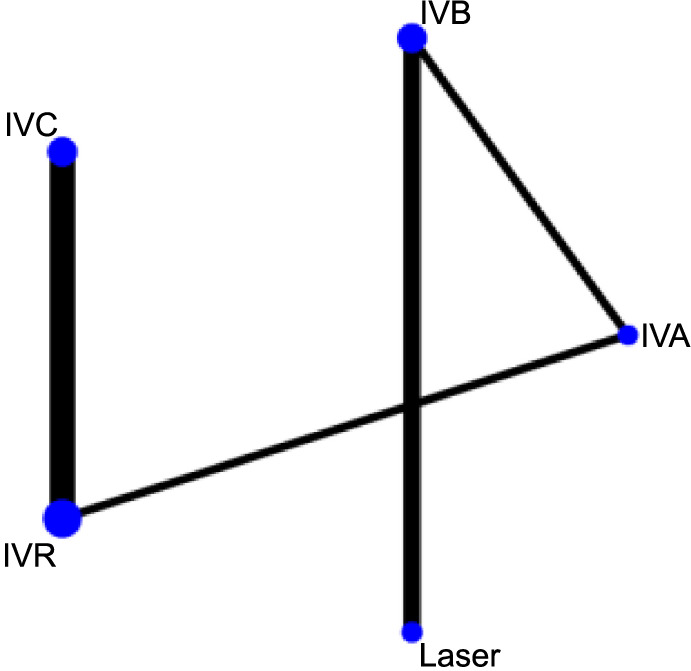
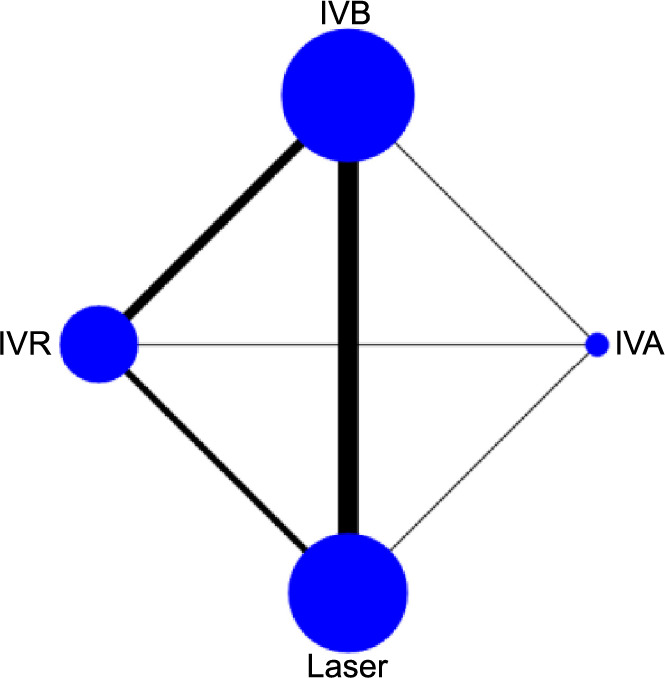
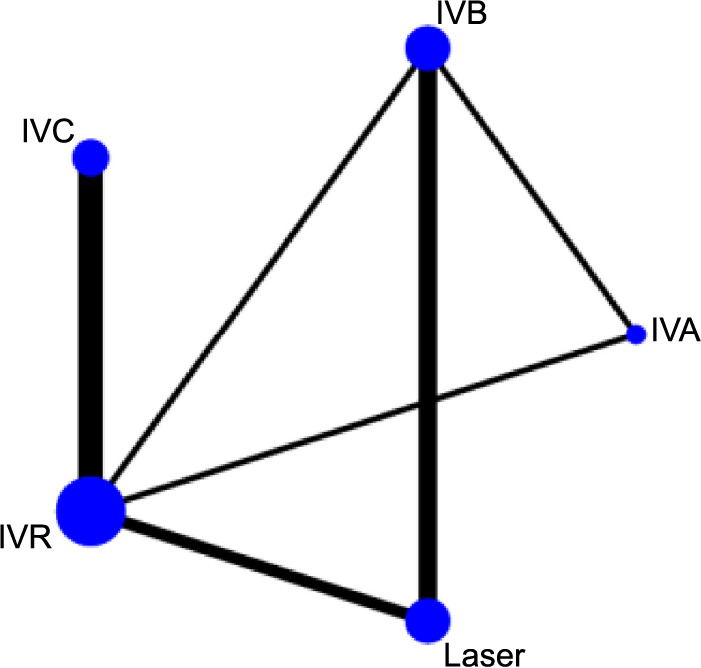
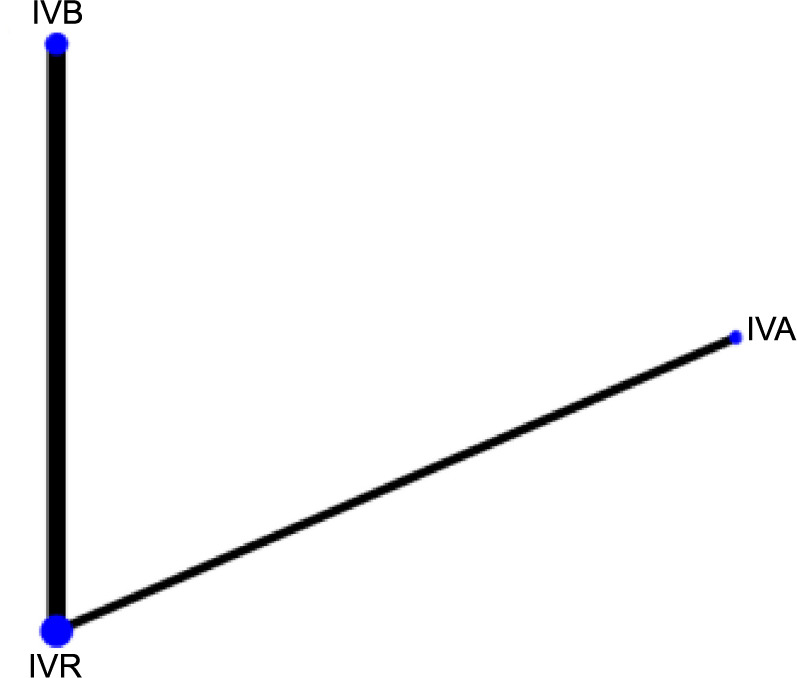
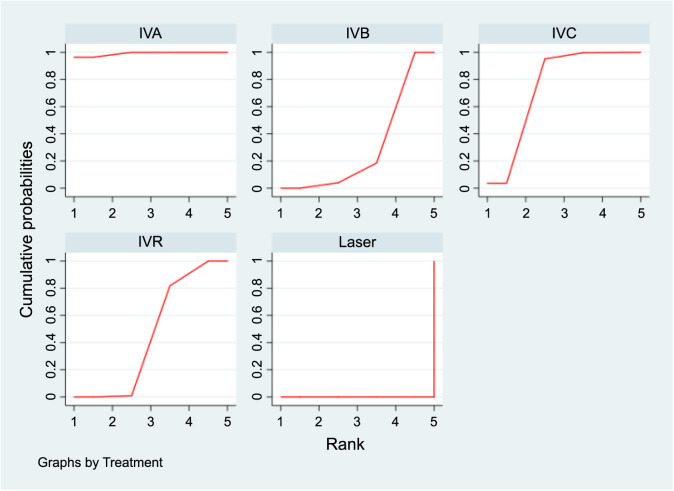
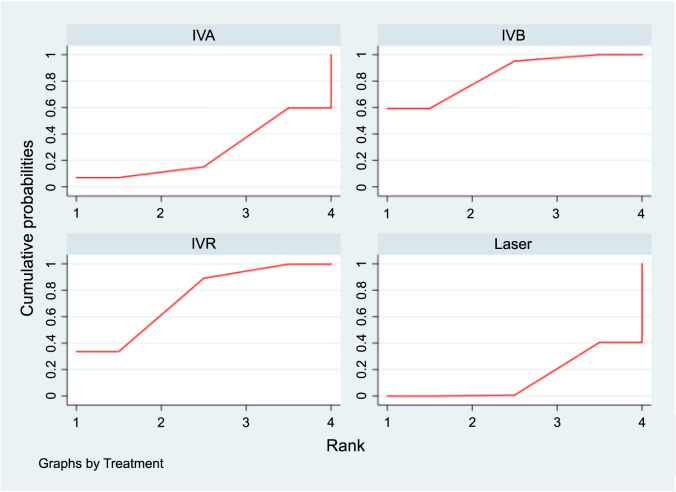
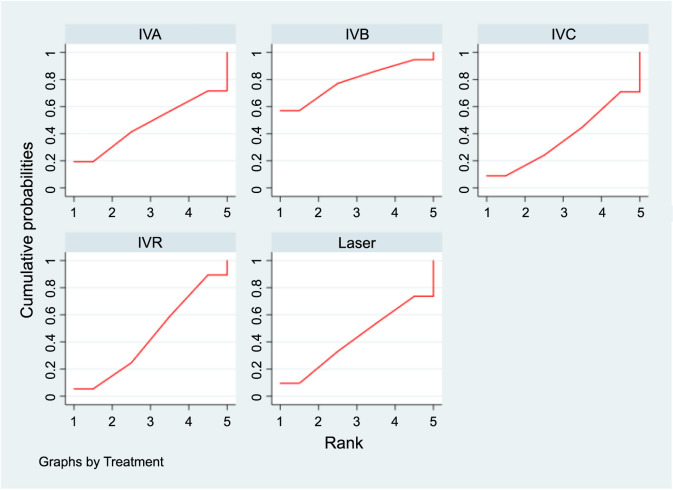
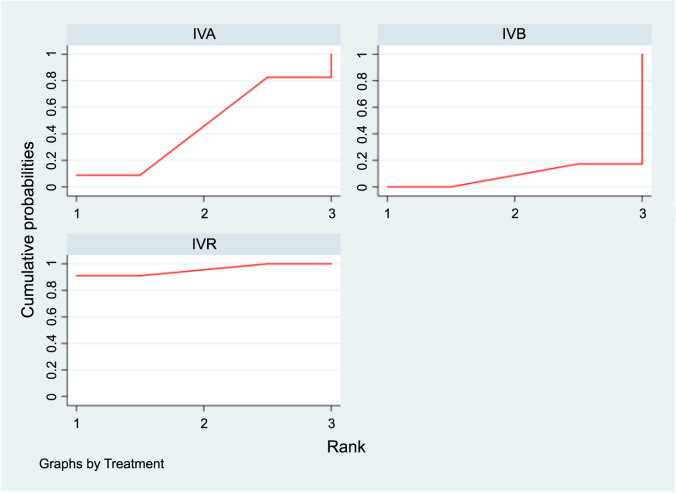
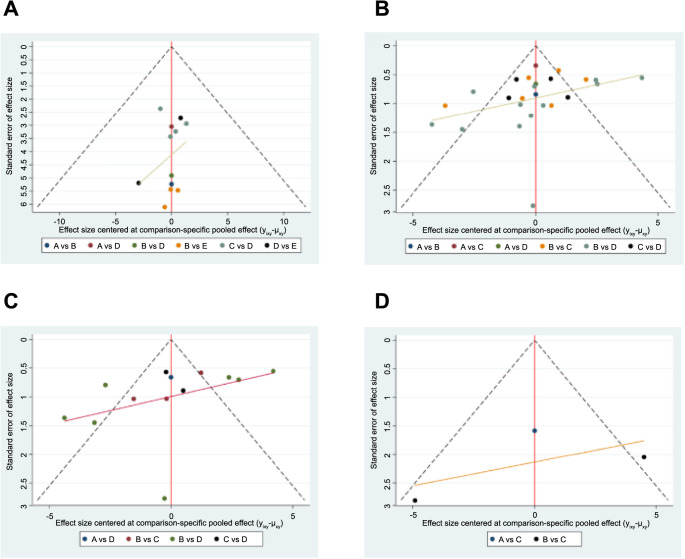
This study undertakes a comprehensive comparison of five different interventions for the treatment of type-1 retinopathy of prematurity (ROP) and aggressive posterior ROP (APROP), offering insights into their relative efficacies and contributing to better clinical decision making. The aim of this study was to compare the efficacy of intravitreal aflibercept (IVA), intravitreal bevacizumab (IVB), intravitreal conbercept (IVC), intravitreal ranibizumab (IVR), and laser therapy in treating these conditions. We conducted a search for relevant randomized controlled trials (RCTs) in databases, namely, PubMed, Embase, Cochrane Library, Web of Science, and Ovid, focusing on these five treatment modalities for ROP. The quality of the included studies was evaluated using the Cochrane Risk of Bias Assessment Tool, and data analysis was performed using STATA software. The results from our network meta-analysis (NMA) indicated that IVA significantly prolonged the interval between initial treatment and relapse in patients, with a surface under the cumulative ranking curve (SUCRA) value of 99.1%. Additionally, patients in the IVB group had a significantly higher spherical equivalent refraction (SER) after surgery, with a SUCRA value of 84.4%. Furthermore, IVR was the most effective in reducing the duration of peripheral retinal vascularization, with a SUCRA value of 95.6%. However, no statistically significant differences were found in relapse rates among the five treatment options. Our analysis concludes that intravitreal injections of anti-vascular endothelial growth factor (anti-VEGF) drug monotherapy generally offer better outcomes than laser treatment for ROP. Nonetheless, additional RCTs are necessary to further evaluate the safety of anti-VEGF agents.
Conflict of interest statement
Conflicts of interest: Authors declare no conflicts of interest.
Figures
Similar articles
-
Comparison of different agents and doses of anti-vascular endothelial growth factors (aflibercept, bevacizumab, conbercept, ranibizumab) versus laser for retinopathy of prematurity: A network meta-analysis.Surv Ophthalmol. 2024 Jul-Aug;69(4):585-605. doi: 10.1016/j.survophthal.2024.02.005. Epub 2024 Mar 1. Surv Ophthalmol. 2024. PMID: 38432359
-
Aflibercept to treat retinopathy of prematurity: need for more research.J Perinatol. 2025 Feb;45(2):282-286. doi: 10.1038/s41372-024-01997-1. Epub 2024 May 10. J Perinatol. 2025. PMID: 38730278 Review.
-
Efficacy and Safety of Aflibercept and Ranibizumab in the Treatment of Retinopathy of Prematurity.Clin Ther. 2024 Oct;46(10):773-777. doi: 10.1016/j.clinthera.2024.08.011. Epub 2024 Oct 5. Clin Ther. 2024. PMID: 39368879
-
Comparison of Bevacizumab, Ranibizumab, and Laser Photocoagulation in the Treatment of Retinopathy of Prematurity in Turkey.Curr Eye Res. 2017 Mar;42(3):462-469. doi: 10.1080/02713683.2016.1196709. Epub 2016 Jul 15. Curr Eye Res. 2017. PMID: 27420302
-
Comparison of the Efficacy Between Intravitreal Aflibercept and Laser Photocoagulation in the Treatment of Retinopathy of Prematurity.J Pediatr Ophthalmol Strabismus. 2020 Jan 1;57(1):54-60. doi: 10.3928/01913913-20191104-01. J Pediatr Ophthalmol Strabismus. 2020. PMID: 31972042
Cited by
-
Therapeutic outcomes of ranibizumab for zone ii stage 2 retinopathy of prematurity with plus disease.Jpn J Ophthalmol. 2025 Jul;69(4):543-548. doi: 10.1007/s10384-025-01199-y. Epub 2025 May 16. Jpn J Ophthalmol. 2025. PMID: 40377801 Free PMC article.
-
Comparative effects of progestin-based combination therapy for endometrial cancer or atypical endometrial hyperplasia: a systematic review and network meta-analysis.Front Oncol. 2024 May 3;14:1391546. doi: 10.3389/fonc.2024.1391546. eCollection 2024. Front Oncol. 2024. PMID: 38764577 Free PMC article.
References
-
- Dogra M, Katoch D, Dogra M. An update on retinopathy of prematurity (ROP) Ind J Pediatr. 2017;84(12):930–6. https://doi.org/10.1007/s12098-017-2404-3. - PubMed
-
- Morrison D, Shaffer J, Ying G-S, Binenbaum G. Ocular complications following treatment in the postnatal growth and retinopathy of prematurity (G-ROP) study. J AAPOS. 2018;22(2):128–33. https://doi.org/10.1016/j.jaapos.2017.12.005. - PMC - PubMed
-
- Quimson S. Retinopathy of prematurity: pathogenesis and current treatment options. Neonatal Netw. 2015;34(5):284–7. https://doi.org/10.1891/0730-0832.34.5.284. - PubMed
-
- Tan Q, Christiansen SP, Wang J. Development of refractive error in children treated for retinopathy of prematurity with anti-vascular endothelial growth factor (anti-VEGF) agents: a meta-analysis and systematic review. PLoS One. 2019;14(12):e0225643. https://doi.org/10.1371/journal.pone.0225643. - PMC - PubMed
-
- Chen P, Rossin E, Vavvas D. Aflibercept for retinopathy of prematurity: a systematic review and meta-analysis. Ophthalmic Surg Lasers Imaging Retina. 2021;52(12):673–81. https://doi.org/10.3928/23258160-20211124-01. - PubMed
