

Protocol of the Comparison of Intravesical Therapy and Surgery as Treatment Options (CISTO) study: a pragmatic, prospective multicenter observational cohort study of recurrent high-grade non-muscle invasive bladder cancer
- PMID: 37980511
- PMCID: PMC10657633
- DOI: 10.1186/s12885-023-11605-8
Protocol of the Comparison of Intravesical Therapy and Surgery as Treatment Options (CISTO) study: a pragmatic, prospective multicenter observational cohort study of recurrent high-grade non-muscle invasive bladder cancer
Abstract
Background: Bladder cancer poses a significant public health burden, with high recurrence and progression rates in patients with non-muscle-invasive bladder cancer (NMIBC). Current treatment options include bladder-sparing therapies (BST) and radical cystectomy, both with associated risks and benefits. However, evidence supporting optimal management decisions for patients with recurrent high-grade NMIBC remains limited, leading to uncertainty for patients and clinicians. The CISTO (Comparison of Intravesical Therapy and Surgery as Treatment Options) Study aims to address this critical knowledge gap by comparing outcomes between patients undergoing BST and radical cystectomy.
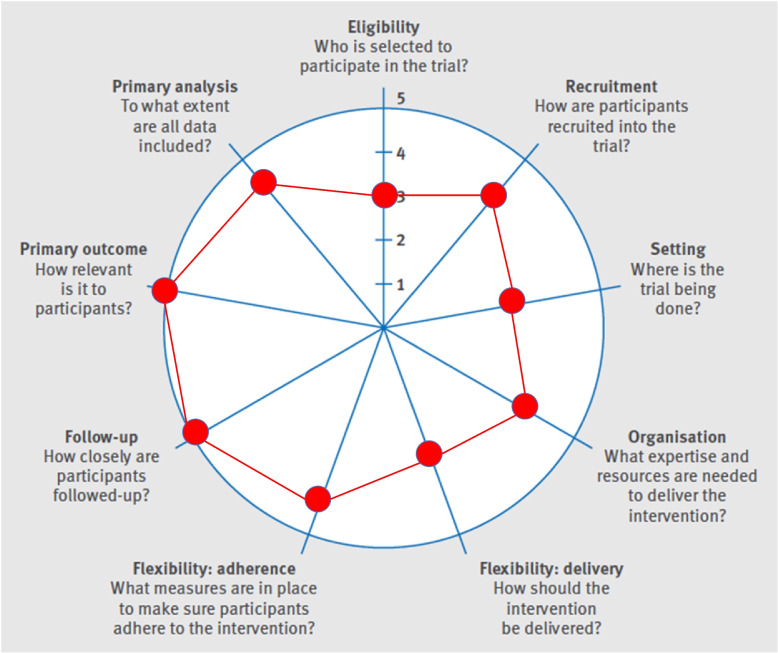
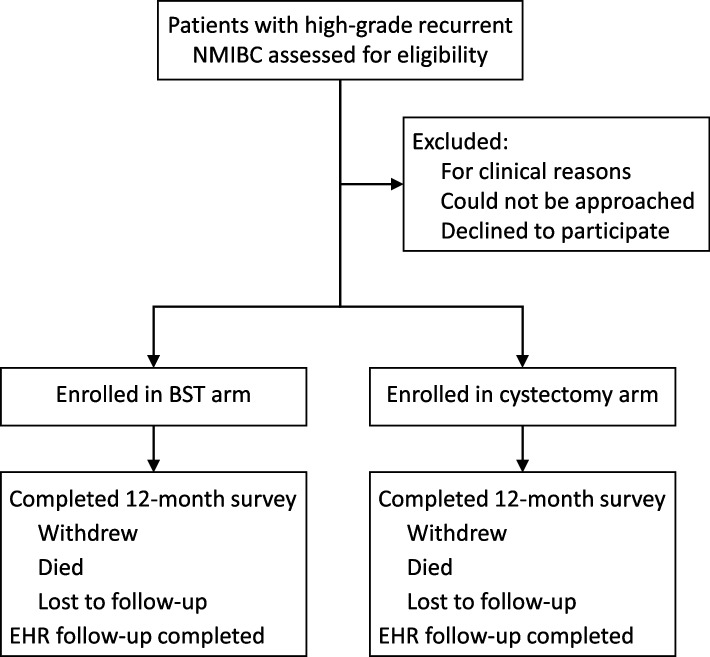
Methods: The CISTO Study is a pragmatic, prospective observational cohort trial across 36 academic and community urology practices in the US. The study will enroll 572 patients with a diagnosis of recurrent high-grade NMIBC who select management with either BST or radical cystectomy. The primary outcome is health-related quality of life (QOL) at 12 months as measured with the EORTC-QLQ-C30. Secondary outcomes include bladder cancer-specific QOL, progression-free survival, cancer-specific survival, and financial toxicity. The study will also assess patient preferences for treatment outcomes. Statistical analyses will employ targeted maximum likelihood estimation (TMLE) to address treatment selection bias and confounding by indication.
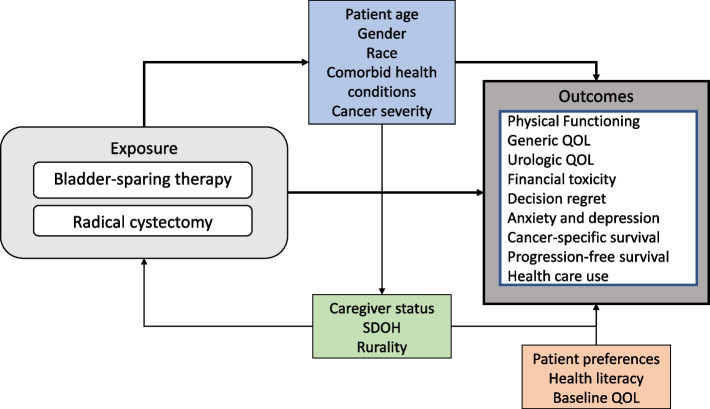
Discussion: The CISTO Study is powered to detect clinically important differences in QOL and cancer-specific survival between the two treatment approaches. By including a diverse patient population, the study also aims to assess outcomes across the following patient characteristics: age, gender, race, burden of comorbid health conditions, cancer severity, caregiver status, social determinants of health, and rurality. Treatment outcomes may also vary by patient preferences, health literacy, and baseline QOL. The CISTO Study will fill a crucial evidence gap in the management of recurrent high-grade NMIBC, providing evidence-based guidance for patients and clinicians in choosing between BST and radical cystectomy. The CISTO study will provide an evidence-based approach to identifying the right treatment for the right patient at the right time in the challenging clinical setting of recurrent high-grade NMIBC.
Trial registration: ClinicalTrials.gov, NCT03933826. Registered on May 1, 2019.
Keywords: Administration, intravesical; Non-muscle invasive bladder cancer; Observational study; Patient-centered care; Pragmatic trial; Quality of life; Radical cystectomy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Associated data
Grants and funding
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
- PCS-2017C3-9380/PCORI/Patient-Centered Outcomes Research Institute/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
