

Nicotinamide mononucleotide impacts HIV-1 infection by modulating immune activation in T lymphocytes and humanized mice
- PMID: 37980794
- PMCID: PMC10694053
- DOI: 10.1016/j.ebiom.2023.104877
Nicotinamide mononucleotide impacts HIV-1 infection by modulating immune activation in T lymphocytes and humanized mice
Abstract
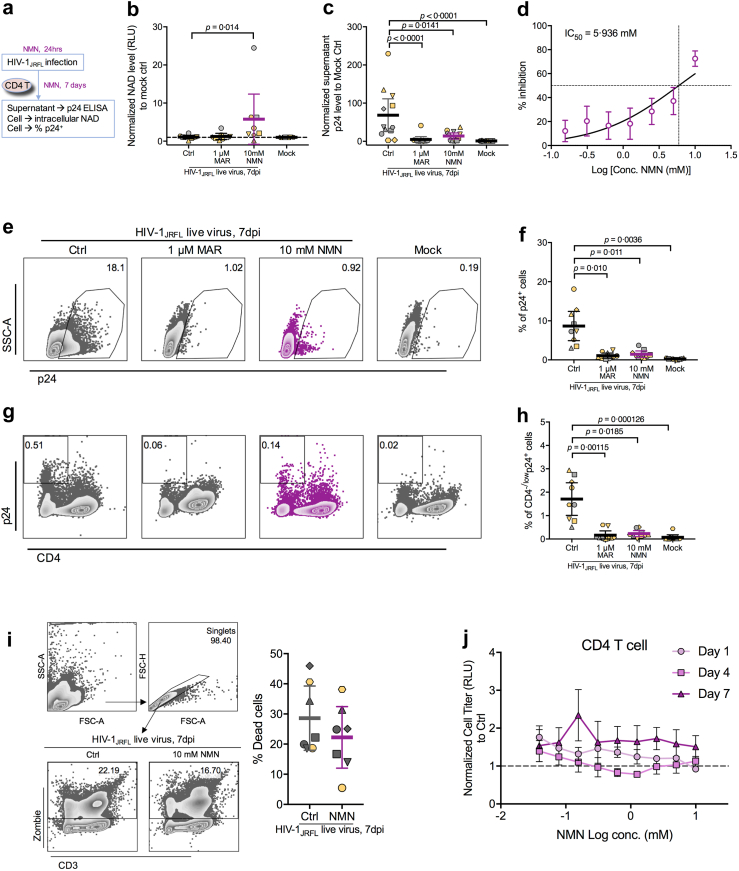
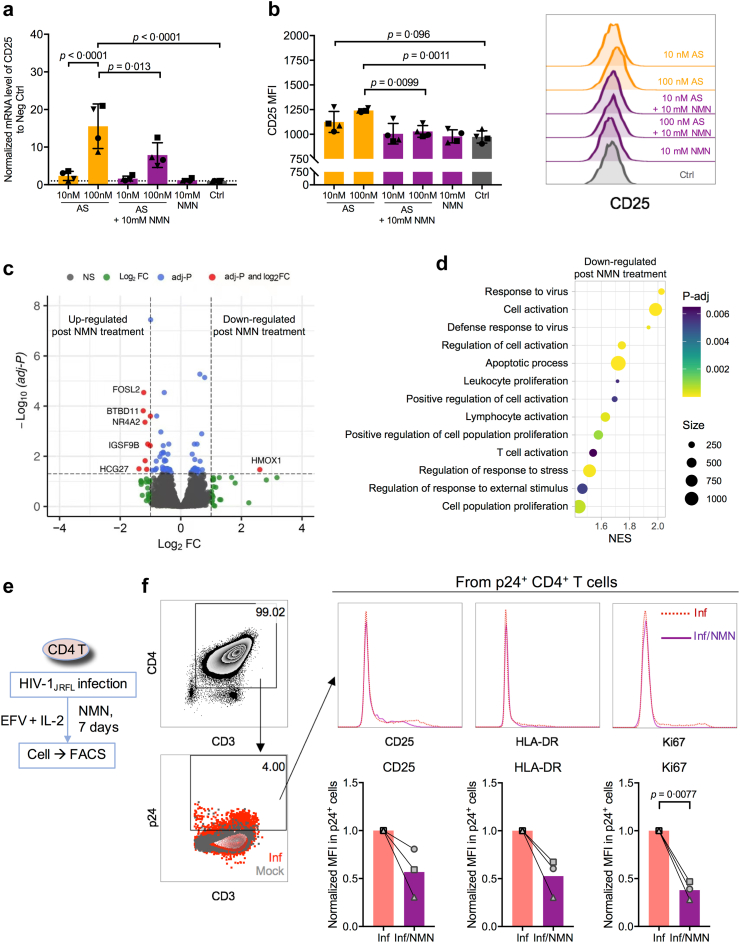
Background: HIV-1-associated immune activation drives CD4+ T cell depletion and the development of acquired immunodeficiency syndrome. We aimed to determine the role of nicotinamide mononucleotide (NMN), the direct precursor of nicotinamide adenine dinucleotide (NAD) co-enzyme, in CD4+ T cell modulation during HIV-1 infection.
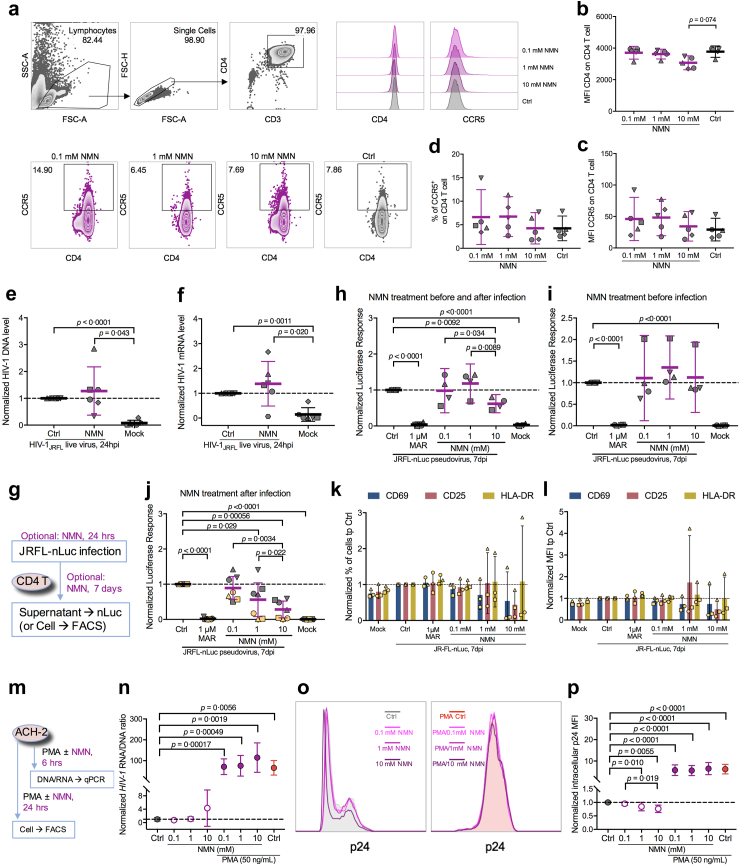
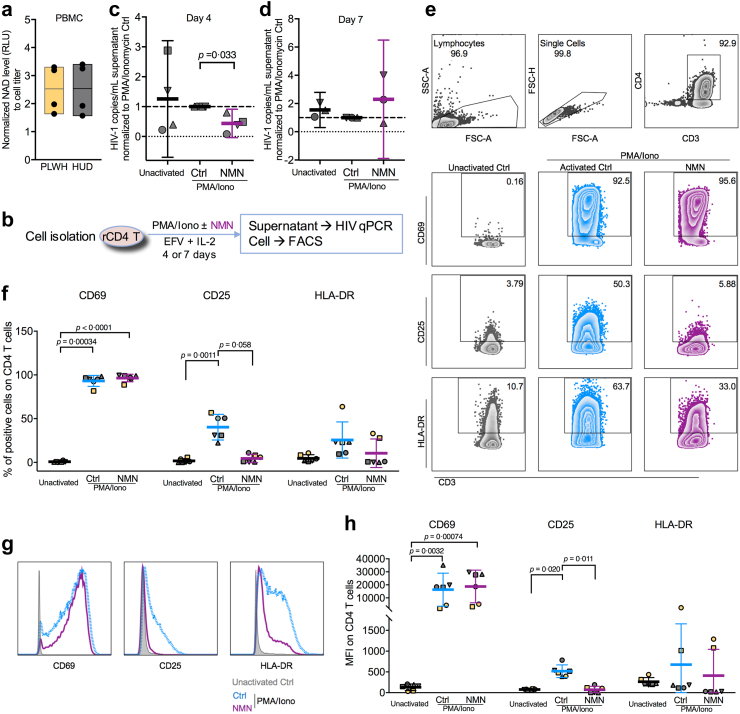
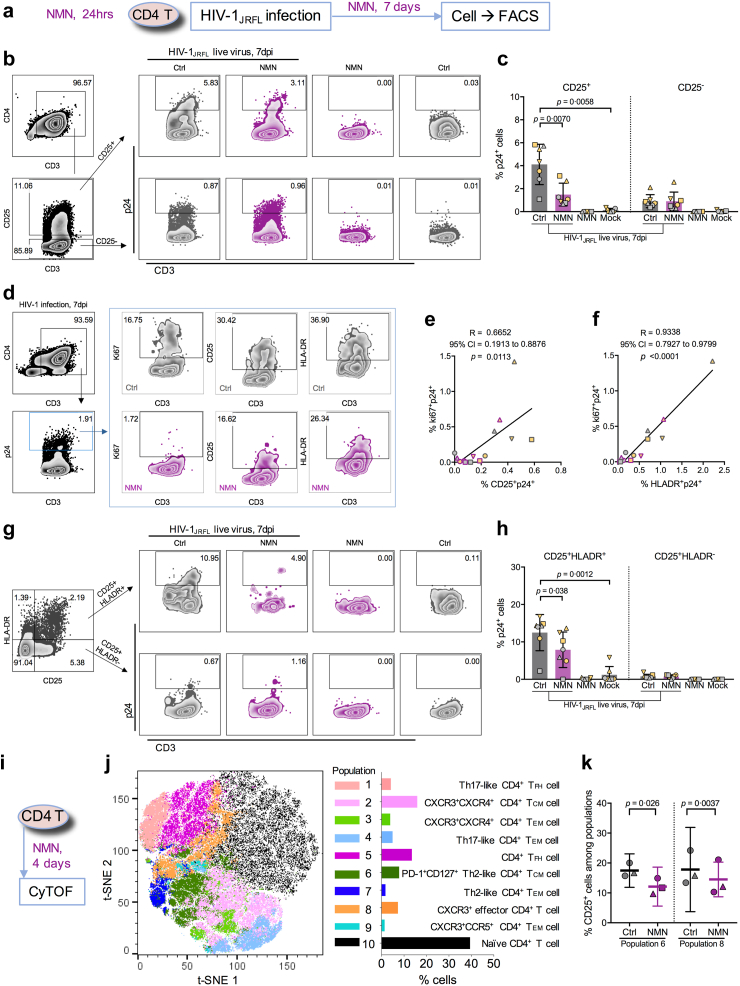
Methods: We examined HIV-1 integrated DNA or transcribed RNA, intracellular p24 protein, and T cell activation markers in CD4+ T cells including in vitro HIV-1-infected cells, reactivated patient-derived cells, and in HIV-1-infected humanized mice, under NMN treatment. RNA-seq and CyTOF analyses were used for investigating the effect of NMN on CD4+ T cells.
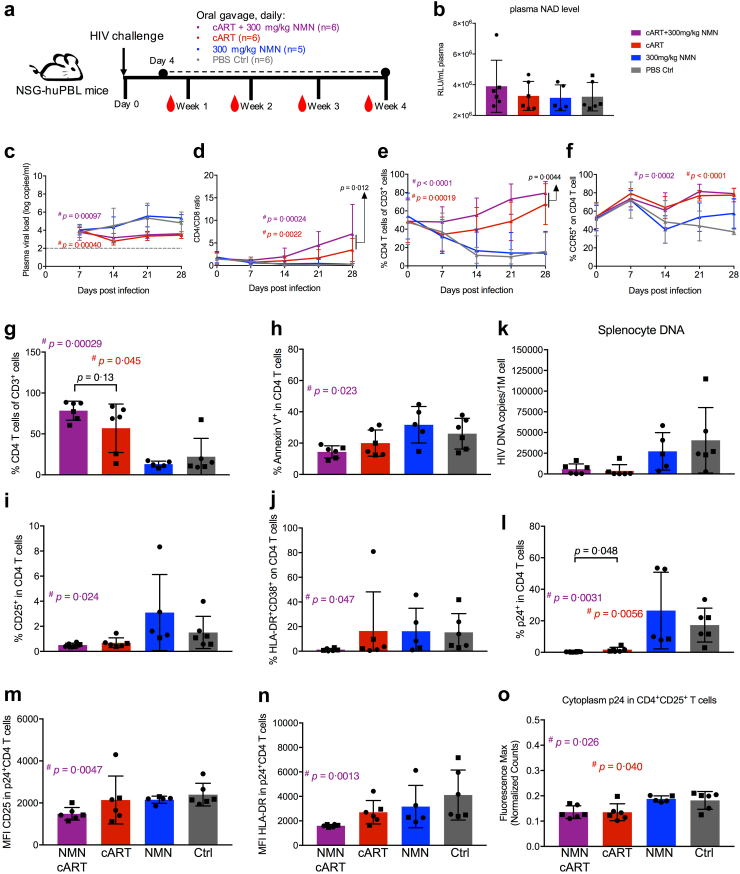
Findings: We found that NMN increased the intracellular NAD amount, resulting in suppressed HIV-1 p24 production and proliferation in infected CD4+ T cells, especially in activated CD25+CD4+ T cells. NMN also inhibited CD25 expression on reactivated resting CD4+ T cells derived from cART-treated people living with HIV-1 (PLWH). In HIV-1-infected humanized mice, the frequency of CD4+ T cells was reconstituted significantly by combined cART and NMN treatment as compared with cART or NMN alone, which correlated with suppressed hyperactivation of CD4+ T cells.
Interpretation: Our results highlight the suppressive role of NMN in CD4+ T cell activation during HIV-1 infection. It warrants future clinical investigation of NMN as a potential treatment in combination with cART in PLWH.
Funding: This work was supported by the Hong Kong Research Grants Council Theme-Based Research Scheme (T11-706/18-N), University Research Committee of The University of Hong Kong, the Collaborative Research with GeneHarbor (Hong Kong) Biotechnologies Limited and National Key R&D Program of China (Grant2021YFC2301900).
Keywords: AIDS; CD4 T cell; HIV-1; Nicotinamide mononucleotide; T cell activation.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests J.W. is an employee and shareholder of GeneHarbor (Hong Kong) Biotechnologies.
Figures
References
-
- Maartens G., Celum C., Lewin S.R. HIV infection: epidemiology, pathogenesis, treatment, and prevention. Lancet. 2014;384(9939):258–271. - PubMed
-
- Gazzola L., Tincati C., Bellistrì G.M., Monforte A., Marchetti G. The absence of CD4+ T cell count recovery despite receipt of virologically suppressive highly active antiretroviral therapy: clinical risk, immunological gaps, and therapeutic options. Clin Infect Dis. 2009;48(3):328–337. - PubMed
-
- Bono V., Augello M., Tincati C., Marchetti G. Failure of CD4+ T-cell recovery upon Virally-effective cART: an enduring gap in the understanding of HIV+ immunological non-responders. New Microbiol. 2022;45(3):155–172. - PubMed
-
- Pirinen E., Auranen M., Khan N.A., et al. Niacin cures systemic NAD(+) deficiency and improves muscle performance in adult-onset mitochondrial myopathy. Cell Metabol. 2020;31(6):1078–1090.e5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
