

Comparing mental health semi-structured diagnostic interviews and symptom checklists to predict poor life outcomes: an 8-year cohort study from childhood to young adulthood in Brazil
- PMID: 37980914
- PMCID: PMC10716620
- DOI: 10.1016/S2214-109X(23)00462-X
Comparing mental health semi-structured diagnostic interviews and symptom checklists to predict poor life outcomes: an 8-year cohort study from childhood to young adulthood in Brazil
Abstract
Background: Semi-structured diagnostic interviews and symptom checklists present similar internal reliability. We aim to investigate whether they differ in predicting poor life outcomes in the transition from childhood to young adulthood.
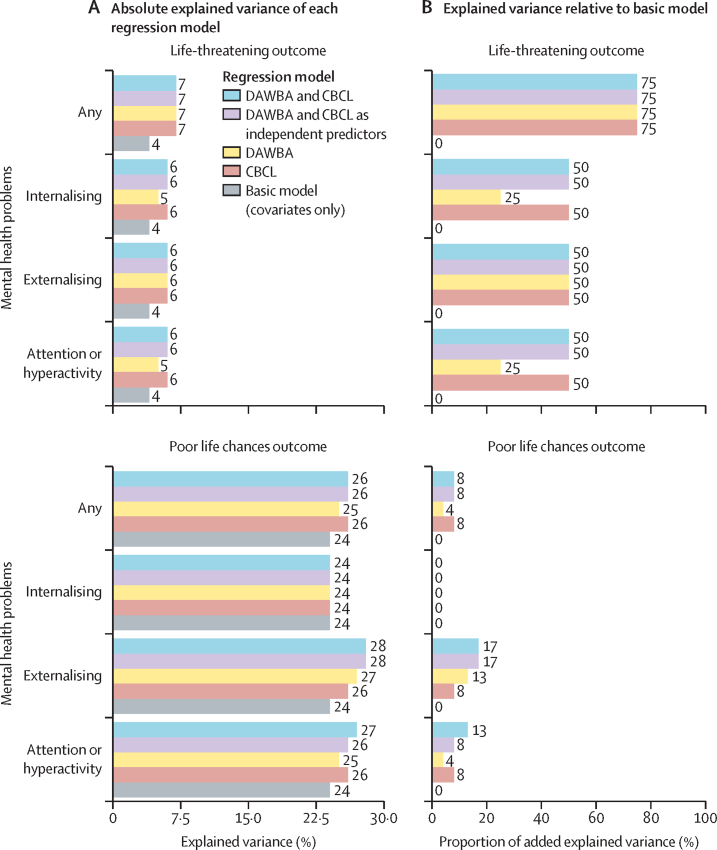
Methods: For this longitudinal study, we used data from the Brazilian High Risk Cohort Study for Childhood Mental Health Conditions. Eligible participants were aged 6-14 years on the day of study enrolment (January to February, 2010) and were enrolled in public schools by a biological parent in Porto Alegre and São Paulo, Brazil. 2511 young people and their caregivers were assessed at baseline in 2010-11, and 1917 were assessed 8 years later (2018-19; 76·3% retention). Clinical thresholds were derived using semi-structured parent-report interview based on the Diagnostic and Statistical Manual of Mental Disorders, according to the Developmental and Well-being Assessment (DAWBA), and clinical scores as defined by the Child Behavior Checklist (CBCL; T-score ≥70 considered positive caseness). At 8 years, participants were assessed for a composite life-threatening outcome (a composite of death, suicide attempts, severe self-harm, psychiatric inpatient admission, or emergency department visits) and a composite poor life chances outcome (a composite of any criminal conviction, substance misuse, or school dropout). We evaluated the accuracy of DAWBA and CBCL to predict these outcomes. Logistic regression models were adjusted for age, sex, race or ethnicity, study site, and socioeconomic class.
Findings: DAWBA and CBCL had similar sensitivity, specificity, predictive values, and test accuracy for both composite outcomes and their components. Any mental health problem, as classified by DAWBA and CBCL, was independently associated with the composite life-threatening outcome (DAWBA adjusted odds ratio 1·62, 95% CI 1·20-2·18; CBCL 1·66, 1·19-2·30), but only CBCL independently predicted poor life chances (1·56, 1·19-2·04). Participants classified by both approaches did not have higher odds of the life-threatening outcome when compared with participants classified by DAWBA or CBCL alone, nor for the poor life chances outcome when compared with those classified by CBCL alone.
Interpretation: Classifying children and adolescents based on a semi-structured diagnostic interview was not statistically different to symptom checklist in terms of test accuracy and predictive validity for relevant life outcomes. Classification based on symptom checklist might be a valid alternative to costly and time-consuming methods to identify young people at risk for poor life outcomes.
Funding: Conselho Nacional de Desenvolvimento Científico e Tecnológico; Fundação de Amparo à Pesquisa do Estado de São Paulo; and Medical Research Council, European Research Council.
Translation: For the Portuguese translation of the abstract see Supplementary Materials section.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests LAR has received grant or research support from the National Council for Scientific and Technological Development (CNPq) and the US National Institutes of Health (grant R01MH120482); authorship royalties from Oxford Press and ArtMed; consulting fees from Adium, Apsen, Medice, Novartis/Sandoz, and Shire/Takeda; served on the speakers' bureau of Abdi Ibrahim, Abbott, Aché, Adium, Apsen, Bial, Medice, Novartis/Sandoz, Pfizer/Upjohn/Viatris, and Shire/Takeda; participated on an advisory board for Adium, Apsen, Medice, Novartis/Sandoz, and Shire/Takeda; received support for attending meetings from Stavros Niarchos Foundation; and had a leadership role in the International Association of Child and Adolescent Psychiatry and Allied Disciplines. AG has received grant or research support from, served as a consultant to, and served on the speakers' bureau of Aché, Daiichi-Sankyo, Teva, Lundbeck, Cristalia, and Janssen; and received consulting fees from Teva and Daiichi-Sankyo in the past 3 years. PMP received payment or honoraria for lectures and presentations at educational events from Sandoz, Daiichi Sankyo, Eurofarma, Abbot, Libbs, Instituto Israelita de Pesquisa e Ensino Albert Einstein, and Instituto D'Or de Pesquisa e Ensino. All other authors declare no competing interests.
Figures

Comment in
-
Closing the mental health gap to support good life chances for children and young people.Lancet Glob Health. 2024 Jan;12(1):e10-e11. doi: 10.1016/S2214-109X(23)00519-3. Epub 2023 Nov 16. Lancet Glob Health. 2024. PMID: 37980912 No abstract available.
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Eliciting adverse effects data from participants in clinical trials.Cochrane Database Syst Rev. 2018 Jan 16;1(1):MR000039. doi: 10.1002/14651858.MR000039.pub2. Cochrane Database Syst Rev. 2018. PMID: 29372930 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Incentives for preventing smoking in children and adolescents.Cochrane Database Syst Rev. 2017 Jun 6;6(6):CD008645. doi: 10.1002/14651858.CD008645.pub3. Cochrane Database Syst Rev. 2017. PMID: 28585288 Free PMC article.
-
Interventions to improve inhaler technique for people with asthma.Cochrane Database Syst Rev. 2017 Mar 13;3(3):CD012286. doi: 10.1002/14651858.CD012286.pub2. Cochrane Database Syst Rev. 2017. PMID: 28288272 Free PMC article.
Cited by
-
Multitrait GWAS of non-suicidal self-injury and the polygenetic effects on child psychopathology and brain structures.Cell Rep Med. 2025 May 20;6(5):102119. doi: 10.1016/j.xcrm.2025.102119. Epub 2025 May 9. Cell Rep Med. 2025. PMID: 40347941 Free PMC article.
-
The interplay between ADHD and school shift on educational outcomes in children and adolescents: A cross-sectional and longitudinal analysis.Res Sq [Preprint]. 2024 May 13:rs.3.rs-4364073. doi: 10.21203/rs.3.rs-4364073/v1. Res Sq. 2024. Update in: Eur Child Adolesc Psychiatry. 2025 May 29. doi: 10.1007/s00787-025-02758-x. PMID: 38798441 Free PMC article. Updated. Preprint.
-
The interplay between ADHD and school shift on educational outcomes in children and adolescents: a cross-sectional and longitudinal analysis.Eur Child Adolesc Psychiatry. 2025 May 29. doi: 10.1007/s00787-025-02758-x. Online ahead of print. Eur Child Adolesc Psychiatry. 2025. PMID: 40439742
-
Equivalence of psychiatric structured interviews and symptom checklists in predicting health-related quality of life in children with chronic physical illness.Qual Life Res. 2025 May 29. doi: 10.1007/s11136-025-03999-8. Online ahead of print. Qual Life Res. 2025. PMID: 40439818
References
-
- Salum GA, Mogg K, Bradley BP, et al. Threat bias in attention orienting: evidence of specificity in a large community-based study. Psychol Med. 2013;43:733–745. - PubMed
-
- Markon KE, Chmielewski M, Miller CJ. The reliability and validity of discrete and continuous measures of psychopathology: a quantitative review. Psychol Bull. 2011;137:856–879. - PubMed
-
- Zachar P, Kendler KS. The philosophy of nosology. Annu Rev Clin Psychol. 2017;13:49–71. - PubMed
-
- Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development. Lancet. 2018;392:1553–1598. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
