

Motor Rehabilitation Provides Modest Functional Benefits After Intracerebral Hemorrhage: a Systematic Review and Meta-Analysis of Translational Rehabilitation Studies
- PMID: 37981635
- PMCID: PMC11976355
- DOI: 10.1007/s12975-023-01205-w
Motor Rehabilitation Provides Modest Functional Benefits After Intracerebral Hemorrhage: a Systematic Review and Meta-Analysis of Translational Rehabilitation Studies
Abstract
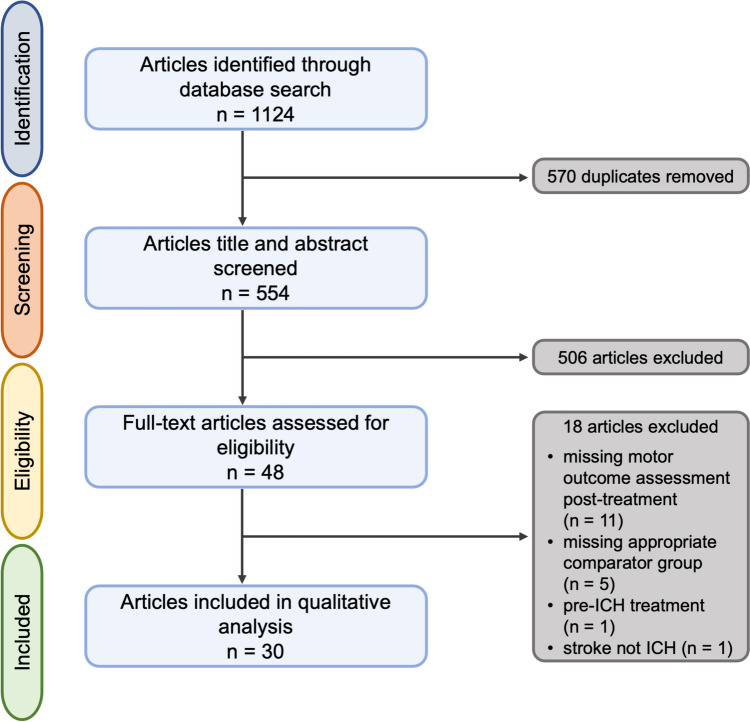
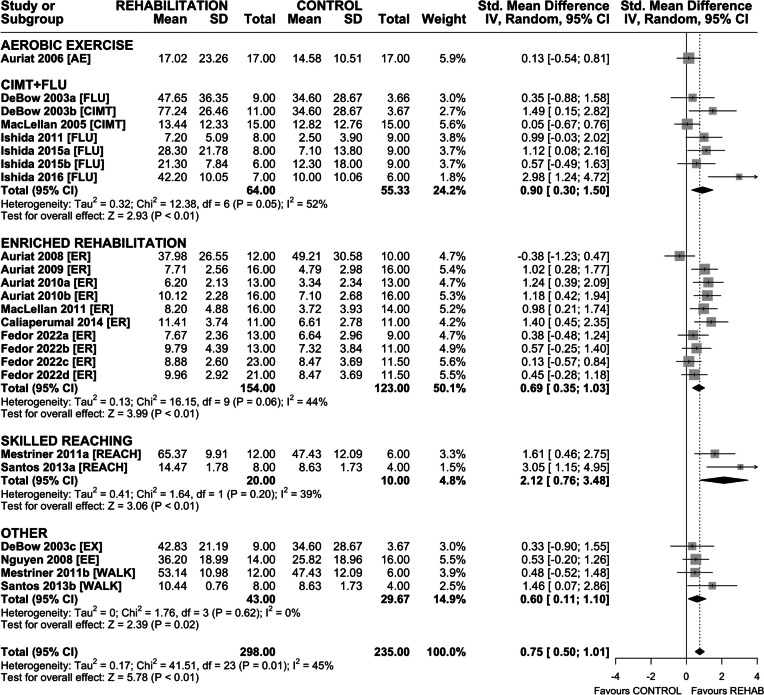
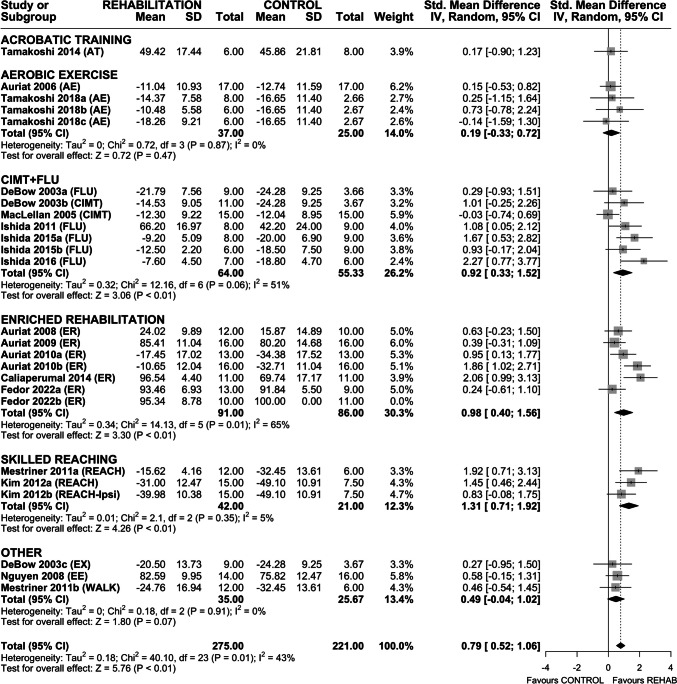
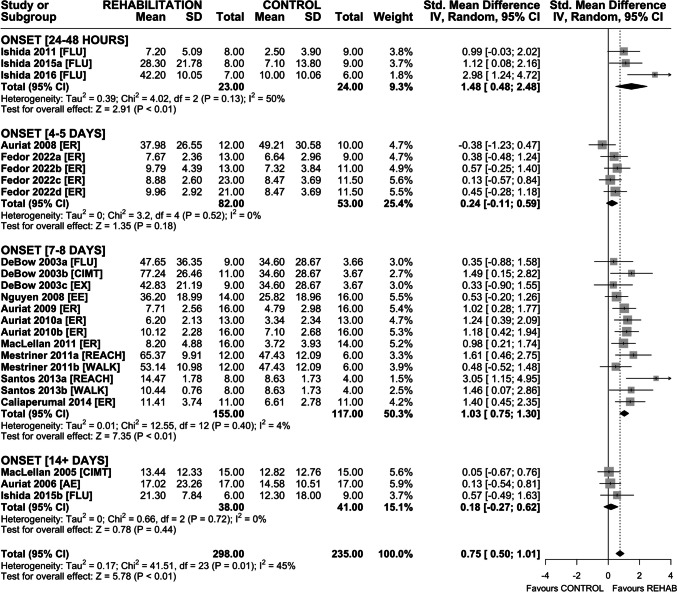
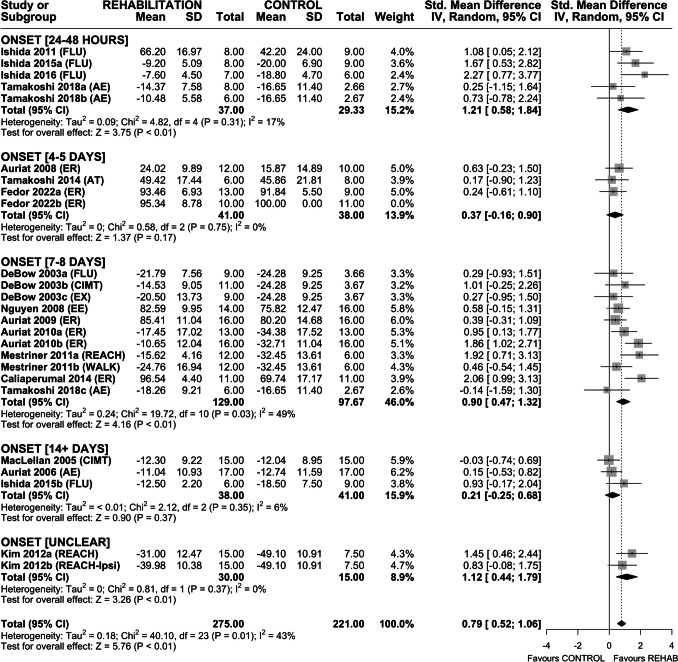
Few certainties exist regarding the optimal type, timing, or dosage of rehabilitation after stroke. Despite differing injury mechanisms and recovery patterns following ischemic and hemorrhagic stroke, most translational stroke research is conducted after ischemia. As we enter the era of personalized medicine, exploring subtype-specific treatment efficacy is essential to optimizing recovery. Our objective was to characterize common rehabilitation interventions used after in vivo preclinical intracerebral hemorrhage (ICH) and assess the impact of post-ICH rehabilitation (vs. no-rehabilitation) on recovery of motor function. Following PRISMA guidelines, a systematic review (Academic Search Complete, CINAHL, EMBASE, Medline, PubMed Central) identified eligible articles published up to December 2022. Risk of bias (SYRCLE) and study quality (CAMARADES) were evaluated, and random-effects meta-analysis was used to assess treatment efficacy in recovery of forelimb and locomotor functions. Thirty articles met inclusion criteria, and 48 rehabilitation intervention groups were identified. Most used collagenase to model striatal ICH in young, male rodents. Aerobic exercise, enriched rehabilitation, and constraint-induced movement therapy represented ~ 70% of interventions. Study quality was low (median 4/10, range 2-8), and risk of bias was unclear. Rehabilitation provided modest benefits in skilled reaching, spontaneous impaired forelimb use, and locomotor function; however, effects varied substantially by endpoint, treatment type, and study quality. Rehabilitation statistically improves motor function after preclinical ICH, but whether these effects are functionally meaningful is unclear. Incomplete reporting and variable research quality hinder our capacity to analyze and interpret how treatment factors influence rehabilitation efficacy and recovery after ICH.
Keywords: Intracerebral hemorrhage; Meta-analysis; Motor recovery; Rehabilitation; Stroke; Translational research.
© 2023. The Author(s).
Conflict of interest statement
Declarations. Ethical Approval: Not applicable. Conflict of Interest: The authors declare no competing interests.
Figures



References
-
- Morovatdar N, Avan A, Azarpazhooh MR, Di Napoli M, Stranges S, Kapral MK, et al. Secular trends of ischaemic heart disease, stroke, and dementia in high-income countries from 1990 to 2017: the Global Burden of Disease Study 2017. Neurol Sci. 2022;43:255–64. - PubMed
-
- Hong K-S, Saver JL. Years of disability-adjusted life gained as a result of thrombolytic therapy for acute ischemic stroke. Stroke. 2010;41:471–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous