

Characterisation of coronary microvascular dysfunction in patients with severe aortic stenosis undergoing TAVI
- PMID: 37982178
- PMCID: PMC10905195
- DOI: 10.4244/EIJ-D-23-00735
Characterisation of coronary microvascular dysfunction in patients with severe aortic stenosis undergoing TAVI
Abstract
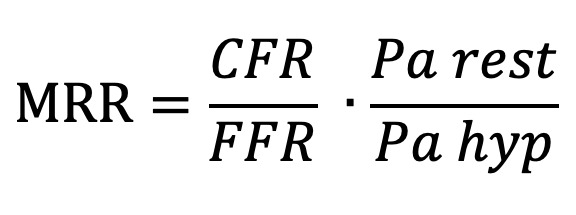
Background: Microvascular resistance reserve (MRR) is a validated measure of coronary microvascular function independent of epicardial resistances.
Aims: We sought to assess whether MRR is associated with adverse cardiac remodelling, a low-flow phenotype and extravalvular cardiac damage (EVCD) in patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI).
Methods: Invasive thermodilution-based assessment of the coronary microvascular function of the left anterior descending artery was performed in a prospective, multicentre cohort of patients undergoing TAVI. Coronary microvascular dysfunction (CMD) was defined as the lowest MRR tertile of the study cohort. Haemodynamic measurements were performed at baseline and then repeated immediately after TAVI. EVCD and markers of a low-flow phenotype were assessed with echocardiography.
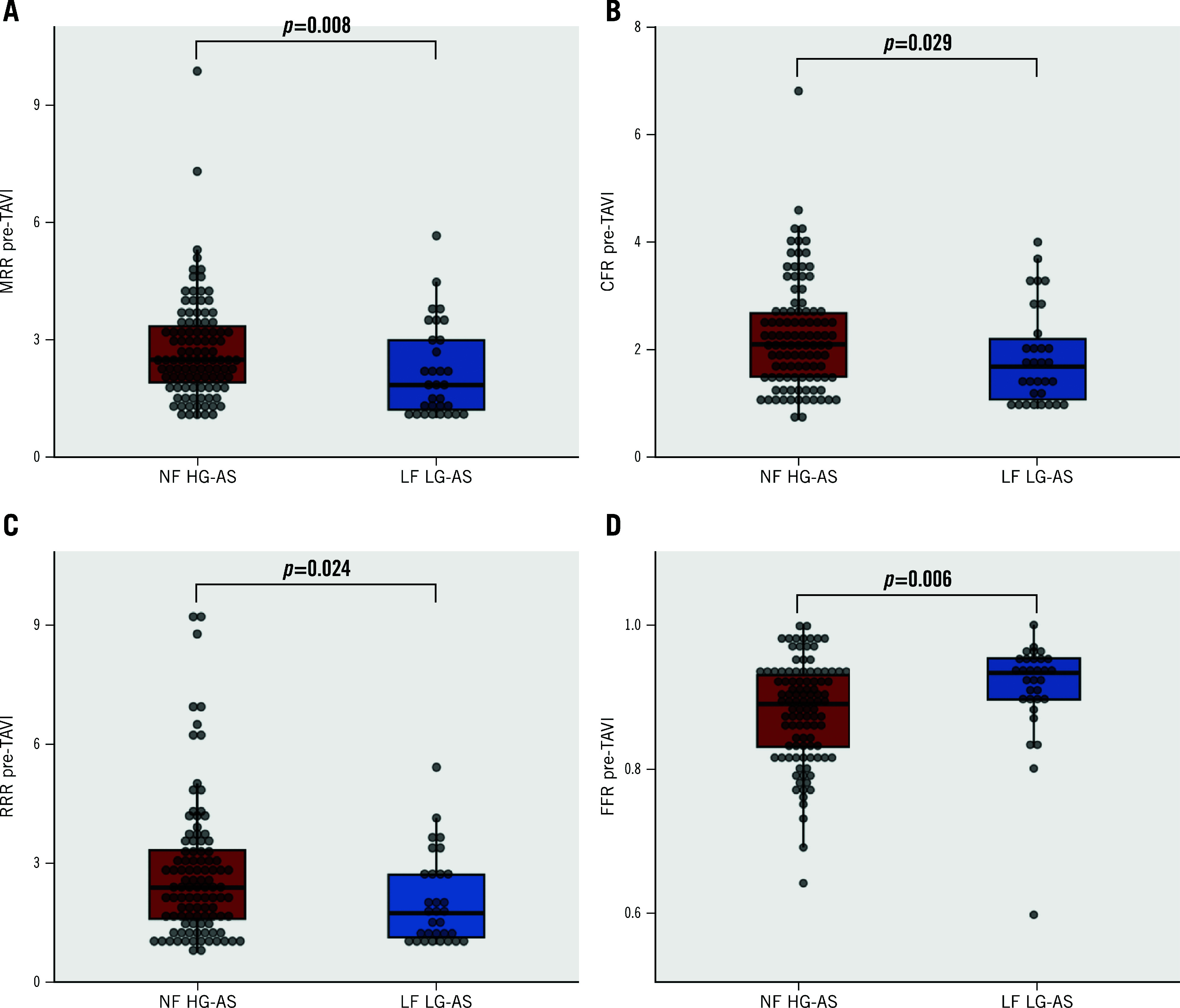
Results: A total of 134 patients were included in this study. Patients with low MRR were more frequently females, had a lower estimated glomerular filtration rate and a higher rate of atrial fibrillation. MRR was significantly lower in patients with advanced EVCD (median 1.80 [1.26-3.30] vs 2.50 [1.87-3.41]; p=0.038) and in low-flow, low-gradient AS (LF LG-AS) (median 1.85 [1.20-3.04] vs 2.50 [1.87-3.40]; p=0.008). Overall, coronary microvascular function tended to improve after TAVI and, in particular, MRR increased significantly after TAVI in the subgroup with low MRR at baseline. However, MRR was significantly impaired in 38 (28.4%) patients immediately after TAVI. Advanced EVCD (adjusted odds ratio 3.08 [1.22-7.76]; p=0.017) and a low-flow phenotype (adjusted odds ratio 3.36 [1.08-10.47]; p=0.036) were significant predictors of CMD.
Conclusions: In this observational, hypothesis-generating study, CMD was associated with extravalvular cardiac damage and a low-flow phenotype in patients with severe AS undergoing TAVI.
Conflict of interest statement
R. Scarsini reports research grant from Abbott and Philips; and speaker fees from Abbott. F. Ribichini reports research grant from Abbott and Philips. P. Paolisso, M. Belmonte, and D.T. Bertolone are supported by a research grant from the CardioPaTh PhD Program. E. Barbato declares speaker fees from Abbott, Boston Scientific, and GE HealthCare. B. De Bruyne has received consultancy fees from Boston Scientific and Abbott; research grants from Coroventis Research, Pie Medical Imaging, CathWorks, Boston Scientific, Siemens, HeartFlow, and Abbott; and owns equity in Siemens, GE HealthCare, Philips, HeartFlow, Edwards Lifesciences, Bayer, Sanofi, and Celiad. M.B. Ancona received consultant fees from Abbott and Abiomed. M. Montorfano is a proctor for Abbott, Kardia, and Boston Scientific. The other authors have no conflicts of interest to declare.
Figures



References
-
- Paolisso P, Gallinoro E, Vanderheyden M, Esposito G, Bertolone DT, Belmonte M, Mileva N, Bermpeis K, De Colle, Fabbricatore D, Candreva A, Munhoz D, Degrieck I, Casselman F, Penicka M, Collet C, Sonck J, Mangiacapra F, de Bruyne, Barbato E. Absolute coronary flow and microvascular resistance reserve in patients with severe aortic stenosis. Heart. 2022;109:47–54. - PubMed
-
- De Bruyne, Pijls NHJ, Gallinoro E, Candreva A, Fournier S, Keulards DCJ, Sonck J, Van’t Veer, Barbato E, Bartunek J, Vanderheyden M, Wyffels E, De Vos, El Farissi, Tonino PAL, Muller O, Collet C, Fearon WF. Microvascular Resistance Reserve for Assessment of Coronary Microvascular Function: JACC Technology Corner. J Am Coll Cardiol. 2021;78:1541–9. - PubMed
-
- Boerhout CKM, Lee JM, de Waard, Mejia-Renteria H, Lee SH, Jung JH, Hoshino M, Echavarria-Pinto M, Meuwissen M, Matsuo H, Madera-Cambero M, Eftekhari A, Effat MA, Murai T, Marques K, Doh JH, Christiansen EH, Banerjee R, Nam CW, Niccoli G, Nakayama M, Tanaka N, Shin ES, Appelman Y, Beijk MAM, van Royen, Knaapen P, Escaned J, Kakuta T, Koo BK, Piek JJ, van de. Microvascular resistance reserve: diagnostic and prognostic performance in the ILIAS registry. Eur Heart J. 2023;44:2862–9. - PMC - PubMed
-
- Généreux P, Pibarot P, Redfors B, Mack MJ, Makkar RR, Jaber WA, Svensson LG, Kapadia S, Tuzcu EM, Thourani VH, Babaliaros V, Herrmann HC, Szeto WY, Cohen DJ, Lindman BR, McAndrew T, Alu MC, Douglas PS, Hahn RT, Kodali SK, Smith CR, Miller DC, Webb JG, Leon MB. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur Heart J. 2017;38:3351–8. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials