

The Role of Lymph Node Dissection in the Management of Upper Urothelial Cancer: A Nodal Status-Based Meta-Analytical Study
- PMID: 37982446
- PMCID: PMC10765198
- DOI: 10.5152/tud.2023.23045
The Role of Lymph Node Dissection in the Management of Upper Urothelial Cancer: A Nodal Status-Based Meta-Analytical Study
Abstract
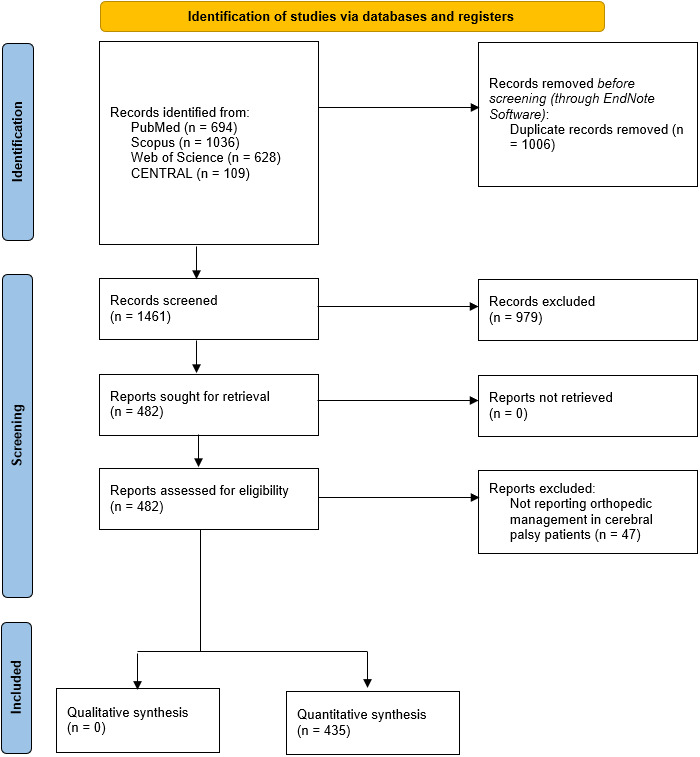
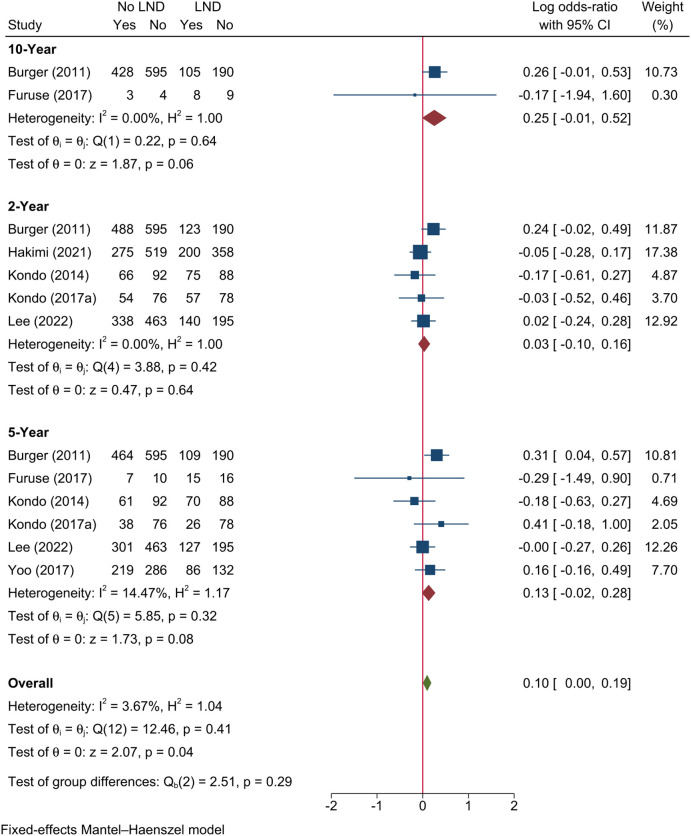
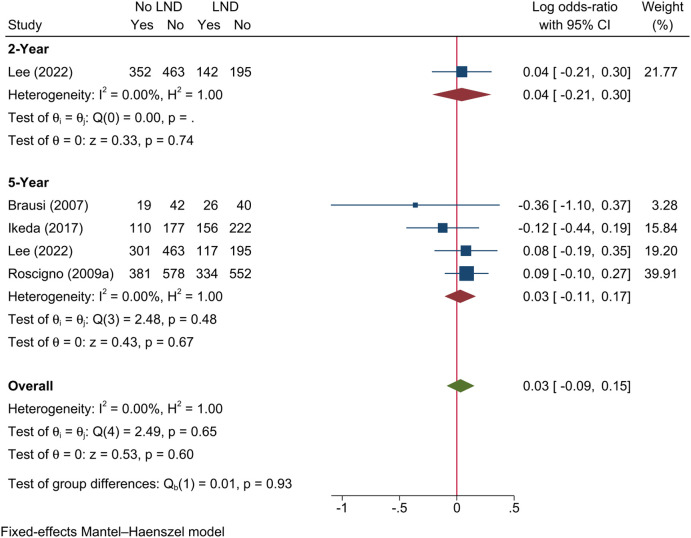
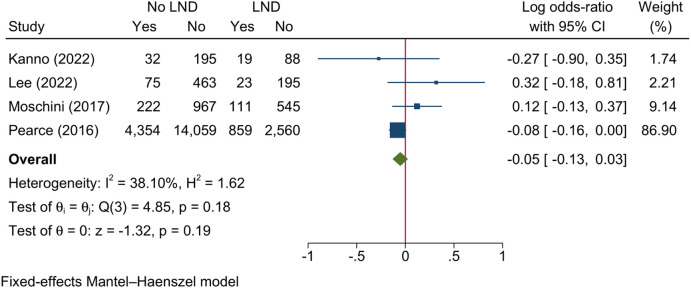
This systematic review was performed to study the prognostic value of lymph node dissection (LND) during nephroureterectomy in upper tract urothelial cancer (UTUC). Five databases were searched on September 11, 2022, to include studies that compared whether LND was performed, the extent of dissection (complete vs. incomplete), and the nodal status (positive "pN+" vs. negative "pN0"). Outcomes included prognosis (overall survival "OS," cancer-specific survival "CSS," disease-free survival "DFS," and recurrence-free survival "RFS") and complications. High-grade complications (≥ grade 3 according to the Clavien-Dindo classification). Data analysis were conducted through STATA. The pooled data are reported log odds ratio (logOR) with 95% CI. Thirty-three studies were analyzed. The LND resulted in improved 5-year OS [logOR=0.10; 95% CI: 0.06-0.15], 5-year CSS [logOR=0.10; 95% CI: 0.04- 0.17], and 10-year CSS [logOR=0.14; 95% CI: 0.06-0.21] when compared to non-LND. However, LND was associated with greater risk of high-grade complications [logOR=0.62; 95% CI: 0.26-0.98]. Complete LND was associated with lower risk of cancer-specific mortality than incomplete LND [logOR=-0.69; 95% CI: -1.22--0.16]. The pN0 patients had better 5-year OS; however, pN+ patients had better prognosis in DFS, RFS (at 2 and 5 years), and CSS (at 2, 5, and 10 years). Lymph node dissection provides a protective role in terms of 5-year OS and 5-year and 10-year CSS among UTUC patients. However, it is associated with higher risk of high-grade complications. The extent of dissection plays a minor prognostic role, while the positivity of resected nodes has great prognostic value in UTUC.
Figures
















References
-
- American Cancer Society. Cancer facts & figures 2022. Available at: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-.... Accessed November 28, 2022.
LinkOut - more resources
Full Text Sources
