

Long-term pulmonary outcome of children with congenital diaphragmatic hernia: functional lung MRI using matrix-pencil decomposition enables side-specific assessment of lung function
- PMID: 37982833
- PMCID: PMC11166819
- DOI: 10.1007/s00330-023-10395-8
Long-term pulmonary outcome of children with congenital diaphragmatic hernia: functional lung MRI using matrix-pencil decomposition enables side-specific assessment of lung function
Abstract
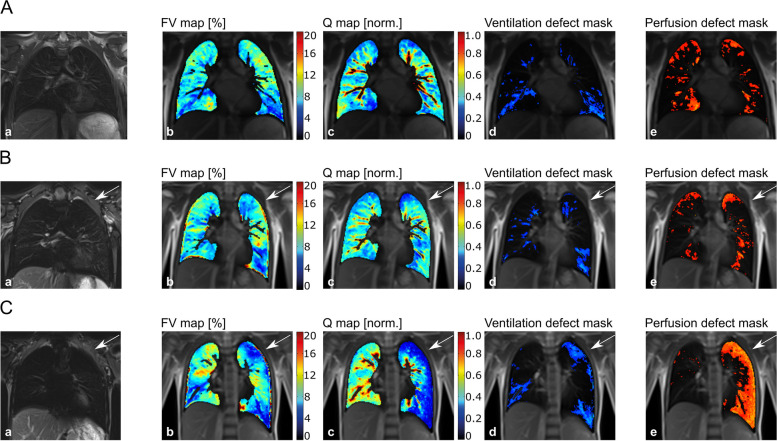
Objectives: In patients with congenital diaphragmatic hernia (CDH) the exact functional outcome of the affected lung side is still unknown, mainly due to the lack of spatially resolved diagnostic tools. Functional matrix-pencil decomposition (MP-) lung MRI fills this gap as it measures side-specific ventilation and perfusion. We aimed to assess the overall and side-specific pulmonary long-term outcomes of patients with CDH using lung function tests and MP-MRI.
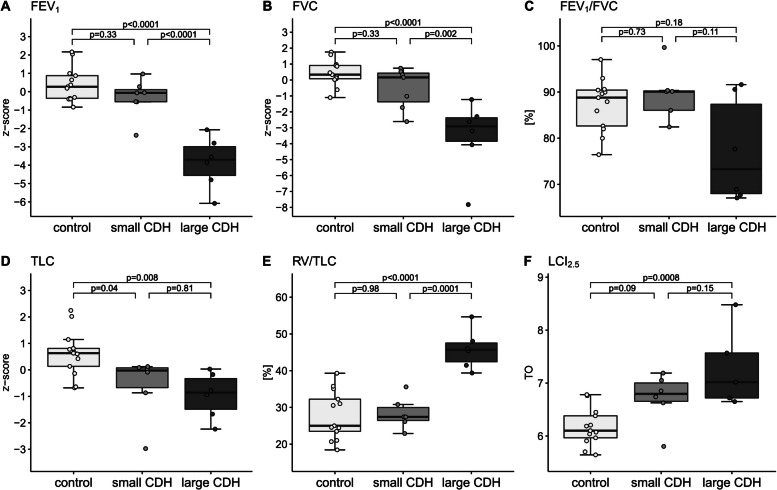
Methods: Thirteen school-aged children with CDH (seven with small and six with large defect-sized CDH, defined as > 50% of the chest wall circumference being devoid of diaphragm tissue) and thirteen healthy matched controls underwent spirometry, multiple-breath washout, and MP-MRI. The main outcomes were forced expiratory volume in 1 second (FEV1), lung clearance index (LCI2.5), ventilation defect percentage (VDP), and perfusion defect percentage (QDP).
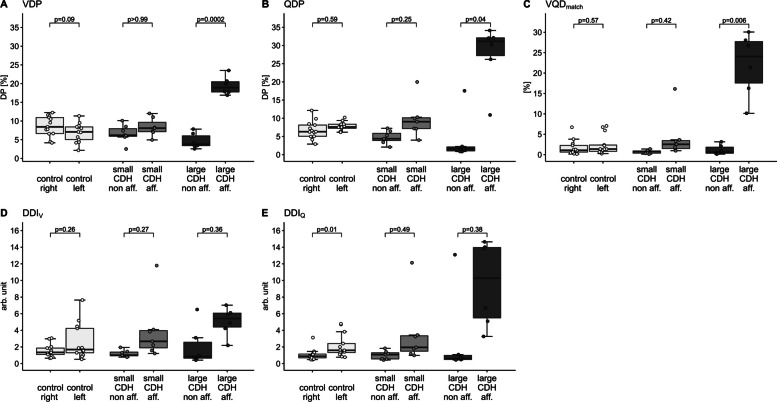
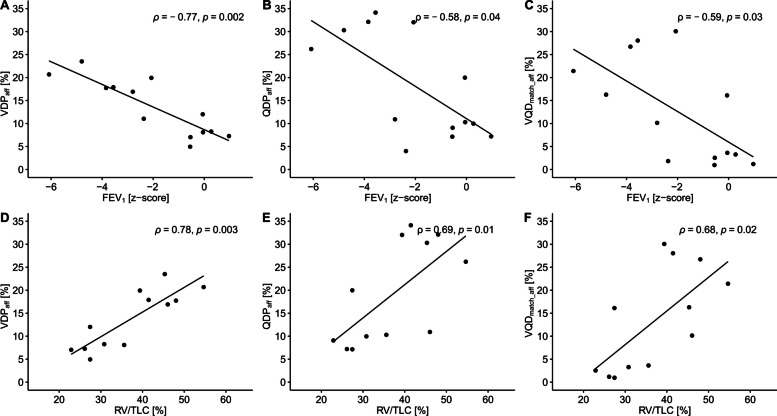
Results: Patients with a large CDH showed significantly reduced overall lung function compared to healthy controls (mean difference [95%-CIadjusted]: FEV1 (z-score) -4.26 [-5.61, -2.92], FVC (z-score) -3.97 [-5.68, -2.26], LCI2.5 (TO) 1.12 [0.47, 1.76], VDP (%) 8.59 [3.58, 13.60], QDP (%) 17.22 [13.16, 21.27]) and to patients with a small CDH. Side-specific examination by MP-MRI revealed particularly reduced ipsilateral ventilation and perfusion in patients with a large CDH (mean difference to contralateral side [95%-CIadjusted]: VDP (%) 14.80 [10.50, 19.00], QDP (%) 23.50 [1.75, 45.20]).
Conclusions: Data indicate impaired overall lung function with particular limitation of the ipsilateral side in patients with a large CDH. MP-MRI is a promising tool to provide valuable side-specific functional information in the follow-up of patients with CDH.
Clinical relevance statement: In patients with congenital diaphragmatic hernia, easily applicable MP-MRI allows specific examination of the lung side affected by the hernia and provides valuable information on ventilation and perfusion with implications for clinical practice, making it a promising tool for routine follow-up.
Key points: • Functional matrix pencil decomposition (MP) MRI data from a small sample indicate reduced ipsilateral pulmonary ventilation and perfusion in children with large congenital diaphragmatic hernia (CDH). • Easily applicable pencil decomposition MRI provides valuable side-specific diagnostic information on lung ventilation and perfusion. This is a clear advantage over conventional lung function tests, helping to comprehensively follow up patients with congenital diaphragmatic hernia and monitor therapy effects.
Keywords: Children; Congenital diaphragmatic hernias; Functional magnetic resonance imaging; Lung; Pulmonary function test.
© 2023. The Author(s).
Conflict of interest statement
Elisabeth Kieninger reports personal fees from Sanofi-Aventis outside the submitted work.
Philipp Latzin reports personal fees from Gilead, Novartis, OM Pharma, Polyphor, Roche, Santhera, Schwabe, Vertex, Vifor, Zambon, and grants from Vertex, all outside the submitted work.
All other authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
