

A Phase Ib First-In-Patient Study Assessing the Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Ponsegromab in Participants with Cancer and Cachexia
- PMID: 37982848
- PMCID: PMC10831332
- DOI: 10.1158/1078-0432.CCR-23-1631
A Phase Ib First-In-Patient Study Assessing the Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Ponsegromab in Participants with Cancer and Cachexia
Abstract
Purpose: Cachexia is common in patients with advanced cancer and is associated with elevated serum growth differentiation factor 15 (GDF-15) concentrations. This first-in-patient (phase Ib), 24-week study assessed use of ponsegromab, a mAb against GDF-15, in adults with advanced cancer, cachexia, and elevated GDF-15 serum concentration.
Patients and methods: Participants (n = 10) received open-label ponsegromab subcutaneous 200 mg every 3 weeks for 12 weeks in addition to standard-of-care anticancer treatment. Ponsegromab safety, tolerability, and pharmacokinetics were assessed in addition to serum GDF-15 concentrations and exploratory measures of efficacy.
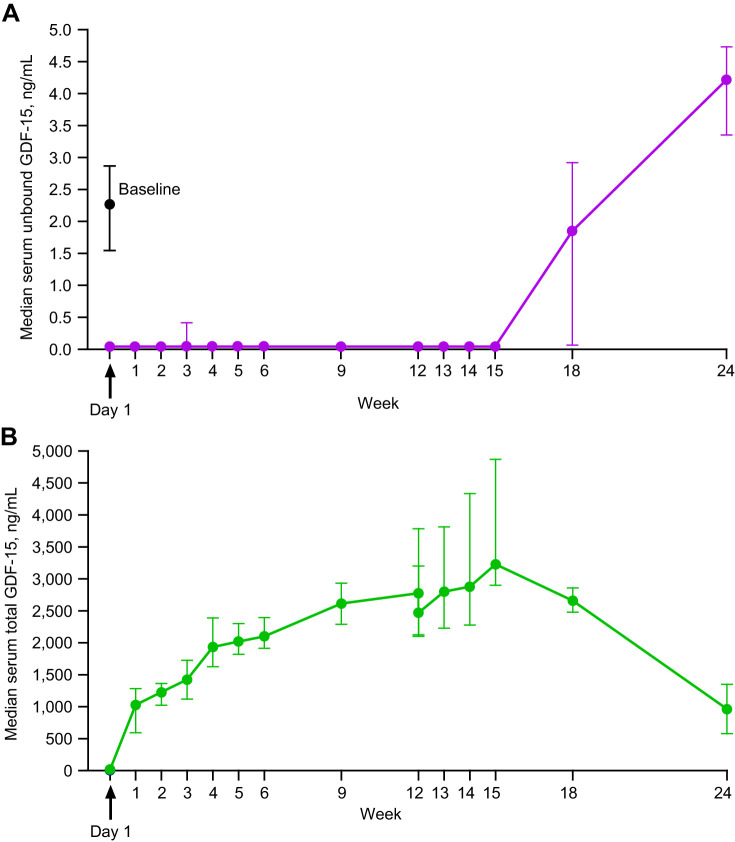
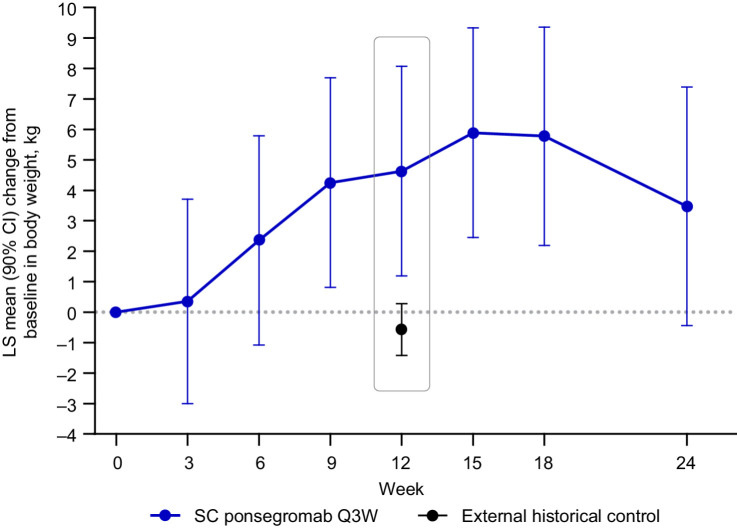
Results: No treatment-related treatment-emergent adverse events, injection site reactions, or adverse trends in clinical laboratory tests, vital signs, or electrocardiogram parameters attributable to ponsegromab were identified. Median serum unbound GDF-15 concentration at baseline was 2.269 ng/mL. Following initiation of study treatment, median unbound GDF-15 concentrations were below the lower limit of quantification (0.0424 ng/mL) from day 1 (3 hours postdose) through week 15. Increases in body weight were observed at all time points during the treatment and follow-up periods. A least-squares mean (SE) increase of 4.63 (1.98) kg was observed at week 12, an increase of approximately 6.6% relative to baseline. Ponsegromab-mediated improvements in actigraphy-based assessments of physical activity and in quality of life, including appetite as assessed by Functional Assessment of Anorexia-Cachexia Therapy total and subscale scores, were also observed.
Conclusions: Ponsegromab was well tolerated, suppressed serum GDF-15 concentrations, and demonstrated preliminary evidence of efficacy. These findings support the continued development of ponsegromab for the treatment of cachexia.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
