

Malignancy in the Upadacitinib Clinical Trials for Rheumatoid Arthritis, Psoriatic Arthritis, Ankylosing Spondylitis, and Non-radiographic Axial Spondyloarthritis
- PMID: 37982966
- PMCID: PMC10796874
- DOI: 10.1007/s40744-023-00621-6
Malignancy in the Upadacitinib Clinical Trials for Rheumatoid Arthritis, Psoriatic Arthritis, Ankylosing Spondylitis, and Non-radiographic Axial Spondyloarthritis
Abstract
Introduction: This article aims to describe malignancies in patients with rheumatoid arthritis (RA), psoriatic arthritis (PsA), ankylosing spondylitis (AS), or non-radiographic axial spondyloarthritis (nr-axSpA) treated with upadacitinib (UPA) or active comparators.
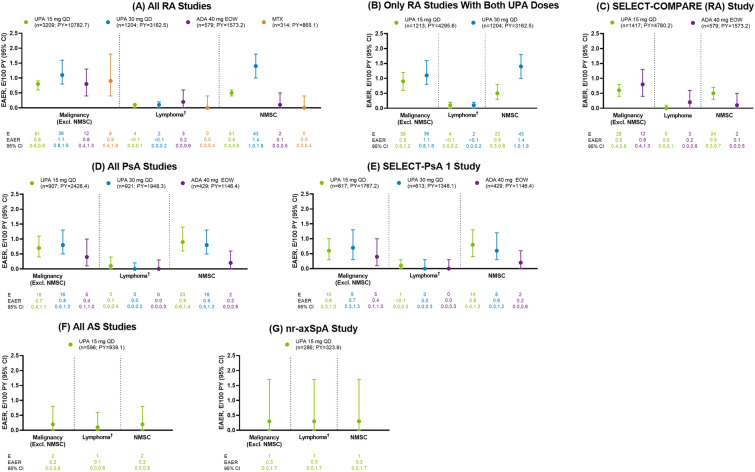
Methods: This integrated safety analysis includes data from 11 phase 3 UPA trials across RA (6 trials), PsA (2 trials), AS (2 trials; one phase 2b/3), and nr-axSpA (1 trial). Treatment-emergent adverse events (TEAEs) were summarized for RA (pooled UPA 15 mg [UPA15], pooled UPA 30 mg [UPA30], adalimumab 40 mg [ADA], methotrexate monotherapy [MTX]), PsA (pooled UPA15, pooled UPA30, ADA), AS (pooled UPA15), and nr-axSpA (UPA15). TEAEs were reported as exposure-adjusted event rates (events/100 patient-years).
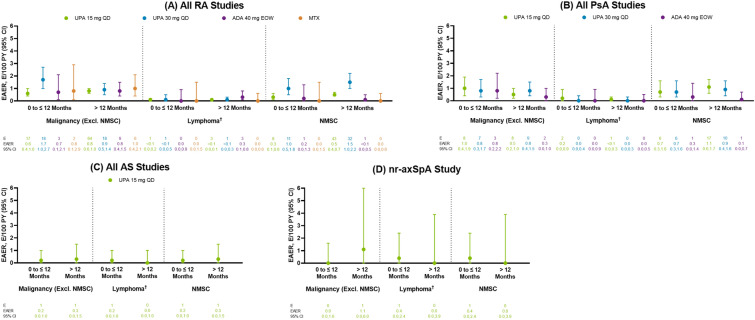
Results: Median treatment duration ranged from 1.0 to 4.0 years (with a maximum of 6.6 years in RA). Across treatments and indications, rates of malignancy excluding nonmelanoma skin cancer (NMSC) ranged from 0.2 to 1.1, while NMSC ranged from 0.0 to 1.4. In RA, rates of malignancy excluding NMSC were generally similar between UPA15, UPA30, ADA, and MTX (breast and lung cancer were the most common). In RA and PsA, Kaplan-Meier analyses revealed no differences in event onset of malignancy excluding NMSC with UPA15 versus UPA30 over time. In RA, NMSC rates were higher with UPA30 than UPA15; both UPA15 and UPA30 were higher than ADA and MTX. In PsA, rates of malignancy excluding NMSC and NMSC were generally similar between UPA15, UPA30, and ADA. In AS and nr-axSpA, malignancies were reported infrequently. Few events of lymphoma were reported across the clinical programs.
Conclusion: Rates of malignancy excluding NMSC were generally similar between UPA15, UPA30, ADA, and MTX and were consistent across RA, PsA, AS, and nr-axSpA. A dose-dependent increased rate of NMSC was observed with UPA in RA.
Trial registration: ClinicaTrials.gov identifier: NCT02706873, NCT02675426, NCT02629159, NCT02706951, NCT02706847, NCT03086343, NCT03104400, NCT03104374, NCT03178487, and NCT04169373.
Keywords: Ankylosing spondylitis (AS); Janus kinase (JAK) inhibitor; Malignancy; Non-radiographic axial spondyloarthritis (nr-axSpA); Nonmelanoma skin cancer (NMSC); Psoriatic arthritis (PsA); Rheumatoid arthritis (RA); Risk factors; Spondyloarthritis (SpA); Upadacitinib (UPA).
© 2023. The Author(s).
Conflict of interest statement
Financial arrangements of the authors with companies whose products may be related to the present manuscript are listed, as declared by the authors. Andrea Rubbert-Roth: Received honoraria for lectures and consulting from AbbVie, Amgen, BMS, Eli Lilly, Gilead, Janssen, MSD, Novartis, Pfizer, Roche, Sanofi, and UCB. Adriana M. Kakehasi: Served as a consultant or member of a speaker’s bureau for, and has received grant/research support from, AbbVie, Amgen, Fresenius Klabi, Janssen, Eli Lilly, Pfizer, Organon, Sandoz, and UCB. Tsutomu Takeuchi: Grant/research support from AbbVie and Eisai; consulting fees from AbbVie, Astellas Pharma, Eli Lilly Japan, and Gilead Sciences; speaker/honoraria from AbbVie, Astellas Pharma, Eisai, Eli Lilly Japan, Gilead Sciences, and Pfizer Japan. Marc Schmalzing: Compensation for consulting from Chugai/Roche, Hexal/Sandoz, Gilead, AbbVie, Janssen-Cilag, Boehringer/Ingelheim, onkowissen.de, EUSA-Pharma, Novartis, AstraZeneca, Amgen, Medac, Lilly, and Galapagos; speaker’s fees from Novartis, AbbVie, AstraZeneca, Chugai/Roche, Janssen-Cilag, Gilead, Boehringer/Ingelheim, Mylan, Galapagos, and EUSA-Pharma; travel grants from Chugai/Roche, Boehringer/Ingelheim, Celgene, Medac, UCB, Mylan, and Galapagos. Hannah Palac: Employee of AbbVie and may hold stock or stock options. Derek Coombs: Employee of AbbVie and may hold stock or stock options. Jianzhong Liu: Employee of AbbVie at time of study and has since retired. May hold stock or stock options in Abbvie. Samuel I. Anyanwu: Employee of AbbVie and may hold stock or stock options. Ralph Lippe: Employee of AbbVie and may hold stock or stock options. Jeffrey R. Curtis: Research grants from AbbVie, Amgen, Bristol Myers Squibb, CorEvitas, Janssen, Labcorp, Lilly, Novartis, Pfizer, Sanofi/Regeneron, and UCB; consulting fees from AbbVie, Amgen, Bristol Myers Squibb, CorEvitas, Janssen, Labcorp, Lilly, Novartis, Pfizer, Sanofi/Regeneron, and UCB.
Figures

References
-
- Bongartz T, Sutton AJ, Sweeting MJ, Buchan I, Matteson EL, Montori V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295:2275–2285. doi: 10.1001/jama.295.19.2275. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
