

Impact of deintensifying hypoglycaemic drugs in older adults with type 2 diabetes: protocol for an emulation of a target trial
- PMID: 37984943
- PMCID: PMC10660441
- DOI: 10.1136/bmjopen-2023-073081
Impact of deintensifying hypoglycaemic drugs in older adults with type 2 diabetes: protocol for an emulation of a target trial
Abstract
Introduction: In older adults with type 2 diabetes (T2D), overtreatment with hypoglycaemic drugs (HDs: sulfonylureas, glinides and/or insulins) is frequent and associated with increased 1-year mortality. Deintensification of HD is thus a key issue, for which evidence is though limited. The primary objective of this study will be to estimate the effect of deintensifying HD on clinical outcomes (hospital admission or death) within 3 months in older adults (≥75 years) with T2D.
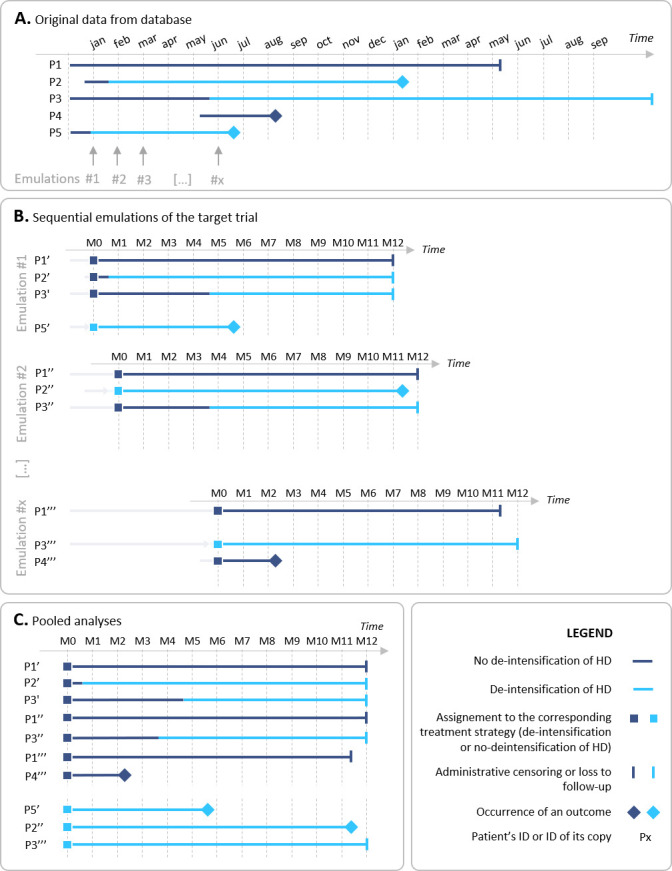
Methods: We will emulate with real-world data a target trial, within The Health Improvement Network cohort, a large-scale database of data collected from electronic medical records of 2000 general practitioners in France. From 1 January 2010 to 28 February 2019, we will include eligible patients ≥75 years who will have T2D, a stable dose of HDs, glycated haemoglobin A1c (HbA1c) value <75 mmol/mol (9.0%) and no deintensification in the past year. The target trial will be sequentially emulated (ie, eligibility assessed) every month in the database. Patients will be classified at baseline of each sequential trial in the intervention arm (deintensification of HDs: decrease of ≥50% in the total dose of HDs, including complete cessation) or control arm (no deintensification of HDs). The pooled dataset for all sequential emulated trials will be analysed. The primary outcome will be time to first occurrence of hospital admission or death, within 3 months. Secondary outcomes will be hospitalisation, death, appropriateness of glycaemic control and occurrence of HbA1c >75 mmol/mol within 1 year. Participants will be followed from baseline to 12 months after randomisation, administrative censoring, or death, whichever occurs first. A pooled logistic regression will be used to estimate the treatment effect on the incidence of the outcomes.
Dissemination and ethics: No ethical approval is needed for using retrospectively this fully anonymised database. The results will be disseminated during conferences and through publications in scientific journals.
Keywords: Aged; CLINICAL PHARMACOLOGY; General diabetes; Patient-Centered Care; Primary Care.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Antoine Christiaens is employed by the Fund for Scientific Research, as a postdoctoral researcher. He received the “Edouard et Lucie Chaffoteaux” Award – 7th edition – from the Société Française de Gériatrie et Gérontologie (SFGG), and the Fondation de France. He received honoraria for a lecture during the Journées de Gériatrie de Nouvelle Aquitaine (Bordeaux, France), from NovoNordisk in April 2022 (This company did not give any guidance, nor did take part in the content of the lecture). He is member of the board of the Belgian Society of Gerontology and Geriatrics (unpaid activity). Florence Tubach is head of the Centre de Pharmacoépidémiologie (Cephepi) of the Assistance Publique – Hôpitaux de Paris and of the Clinical Research Unit of Pitié-Salpêtrière hospital, both these structures have received unrestricted research funding and grants for the research projects handled and fees for consultant activities from a large number of pharmaceutical companies, that have contributed indiscriminately to the salaries of its employees. Florence Tubach is not employed by these structures and did not receive any personal remuneration from these companies. Other authors have no competing interests to declare.
Figures

Similar articles
-
A Qualitative Study of Perspectives of Older Adults on Deintensifying Diabetes Medications.J Gen Intern Med. 2023 Mar;38(4):1008-1015. doi: 10.1007/s11606-022-07828-3. Epub 2022 Sep 29. J Gen Intern Med. 2023. PMID: 36175758 Free PMC article.
-
Head-to-head comparison of intensive lifestyle intervention (U-TURN) versus conventional multifactorial care in patients with type 2 diabetes: protocol and rationale for an assessor-blinded, parallel group and randomised trial.BMJ Open. 2015 Dec 9;5(12):e009764. doi: 10.1136/bmjopen-2015-009764. BMJ Open. 2015. PMID: 26656025 Free PMC article. Clinical Trial.
-
Randomised cross-over trial of vildagliptin and pioglitazone as add-on therapy in patients with type 2 diabetes: predicting Which One is Right Here (WORTH) study protocol.BMJ Open. 2020 Sep 1;10(9):e036518. doi: 10.1136/bmjopen-2019-036518. BMJ Open. 2020. PMID: 32873667 Free PMC article.
-
Psychological interventions to improve self-management of type 1 and type 2 diabetes: a systematic review.Health Technol Assess. 2020 Jun;24(28):1-232. doi: 10.3310/hta24280. Health Technol Assess. 2020. PMID: 32568666 Free PMC article.
-
Sliding scale insulin for non-critically ill hospitalised adults with diabetes mellitus.Cochrane Database Syst Rev. 2018 Nov 29;11(11):CD011296. doi: 10.1002/14651858.CD011296.pub2. Cochrane Database Syst Rev. 2018. PMID: 30488948 Free PMC article.
Cited by
-
Association between hypoglycaemic drug de-intensification, mortality and hospital admission in older adults with type 2 diabetes: a cohort study emulating a target trial.Age Ageing. 2025 May 31;54(6):afaf160. doi: 10.1093/ageing/afaf160. Age Ageing. 2025. PMID: 40499127 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous