

Outcomes of Transjugular Intrahepatic Portosystemic Shunt and Gastric Coronary Vein Embolization for Variceal Bleeding in Cirrhotic Portal Hypertension
- PMID: 37985166
- PMCID: PMC10659130
- DOI: 10.3121/cmr.2023.1796
Outcomes of Transjugular Intrahepatic Portosystemic Shunt and Gastric Coronary Vein Embolization for Variceal Bleeding in Cirrhotic Portal Hypertension
Abstract
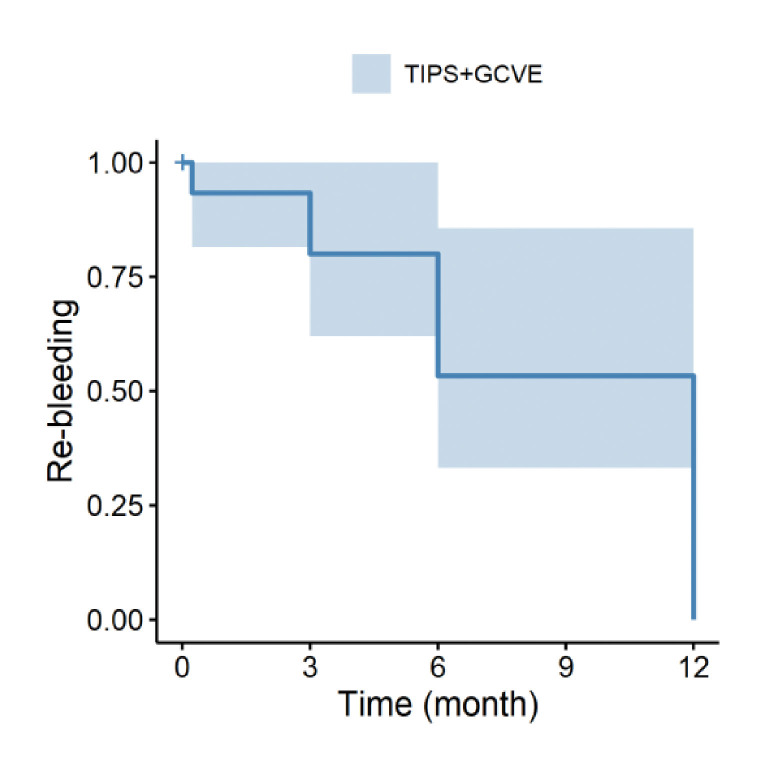
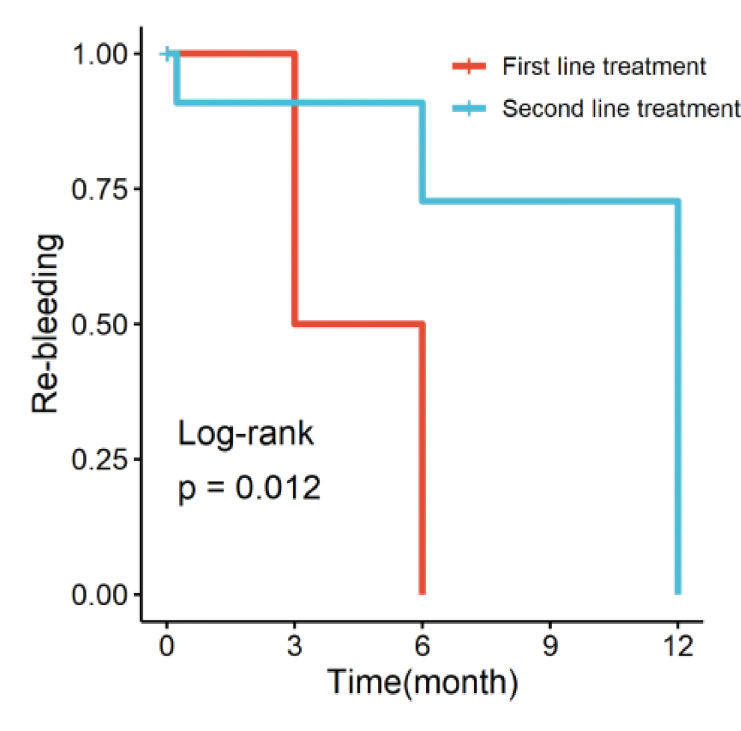
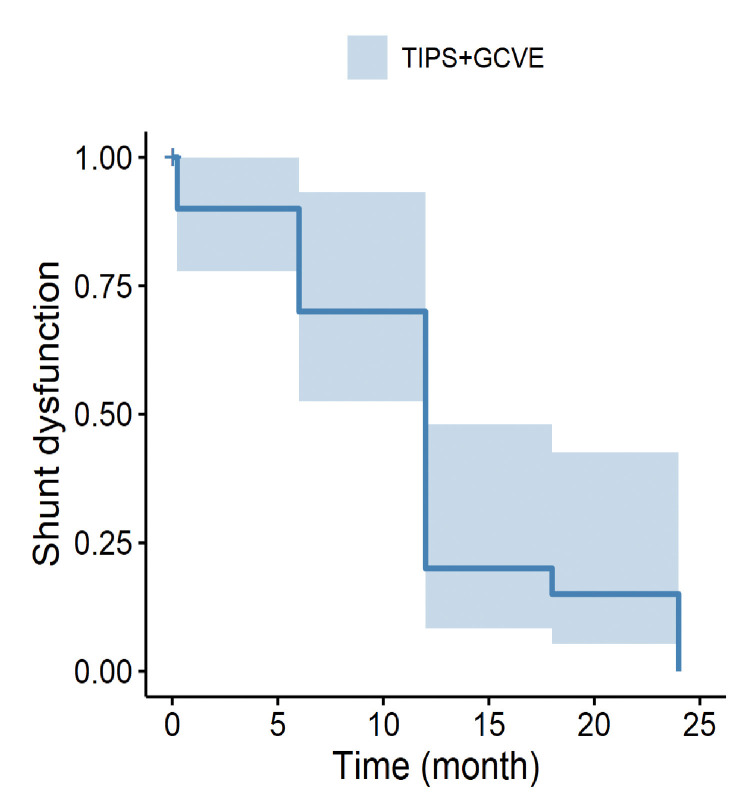
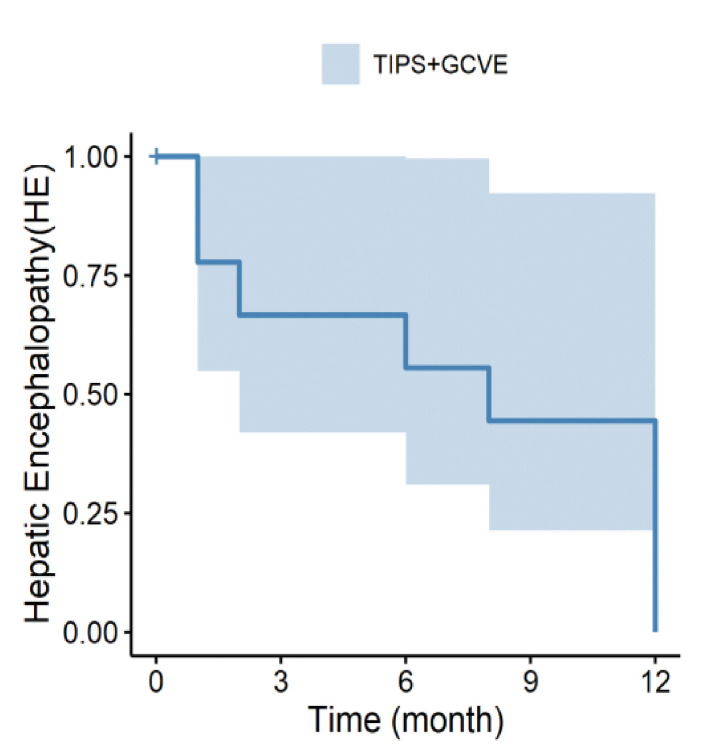
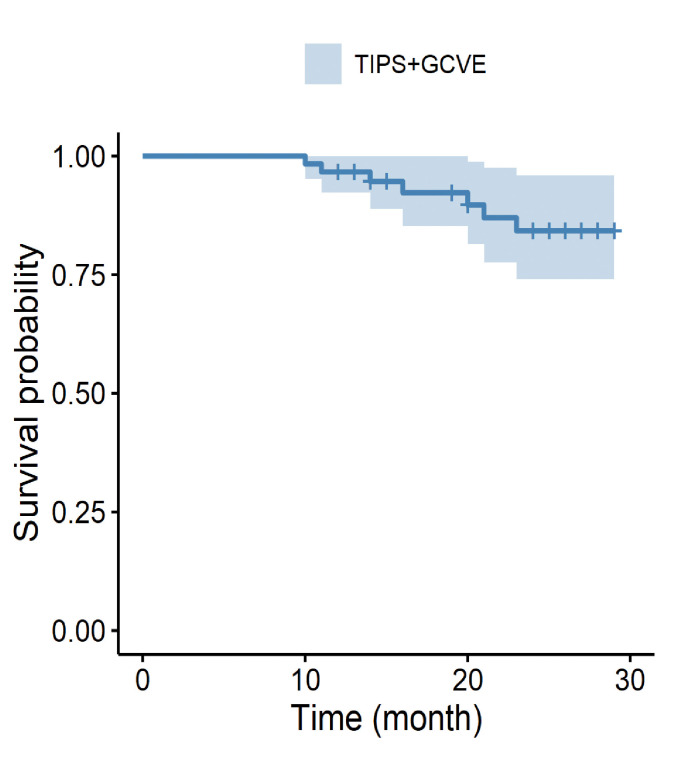
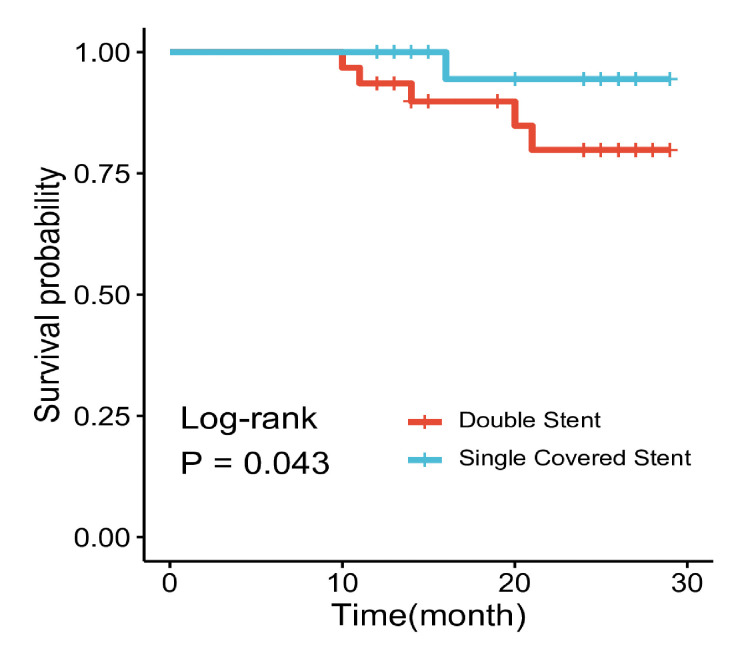
Purpose: To evaluate the efficacy and safety of transjugular intrahepatic portosystemic shunt (TIPS) combined with gastric coronary vein embolization (GCVE) for cirrhotic portal hypertensive variceal bleeding and compare outcomes of first-line with second-line treatment, coil with glue, and single-covered with double stents.Methods: Fifteen patients received TIPS plus GCVE as the first-line treatment for secondary prophylaxis of variceal bleeding, and 45 received it as second-line treatment. Preoperative and postoperative quantitative variables were compared using a paired t test. The incidence of survival rate, re-bleeding, hepatic encephalopathy, and shunt dysfunction were analyzed using the Kaplan-Meier method.Results: The portal venous pressure was significantly decreased from 39.0 ± 5.0 mm Hg to 22.5 ± 4.4 mm Hg (P≤0.001) after TIPS treatment. After 1, 3, 6, 12, 18, and 24 months re-bleeding rates were 1.6%, 3.3%, 6.6%, 13.3%, 0%, and 0%, respectively. Shunt dysfunction rates were 5%, 0%, 10%, 16.6%, 1.6%, and 5%, respectively. Hepatic encephalopathy rates were 3.3%, 1.6%, 3.3%, 6.6%, 0%, and 0%, respectively. And survival rates were 100%, 100%, 100%, 96.6%, 93.3%, and 88.3% respectively. In comparative analysis, statistically significant differences were seen in re-bleeding between the first-line and second-line treatment groups (26.6% vs 24.4%, log-rank P=0.012), and survival rates between single-covered and double stent (3.7% vs 16.1%, log-rang (P=0.043).Conclusion: The results suggest that TIPS combined with GCVE is effective and safer in the treatment of cirrhotic portal hypertensive variceal bleeding. The use of TIP plus GCVE as first-line treatment, may be preferable for high-risk re-bleeding, and more than 25 mm Hg portal venous pressure with repeated variceal bleeding. However, the sample size was small. Therefore, large, randomized, controlled, multidisciplinary center studies are needed for further evaluation.
Keywords: Cirrhotic portal hypertension; Esophageal Variceal bleeding; Gastric Variceal bleeding; Gastric coronary vein embolization; Transjugular intrahepatic portosystemic shunt.
Copyright © 2023 Marshfield Clinic Health System.
Figures
References
-
- Charon JP, Alaeddin FH, Pimpalwar SA, et al. Results of a retrospective multicenter trial of the Viatorr expanded polytetrafluoroethylene-covered stent-graft for transjugular intrahepatic portosystemic shunt creation. J Vasc Interv Radiol. 2004;15(11):1219-1230. doi: 10.1097/01.RVI.0000137434.19522.E5 - DOI - PubMed
-
- Richter GM, Palmaz JC, Nöldge G, et al. Der transjuguläre intrahepatische portosystemische Stent-Shunt (TIPSS). Eine neue nichtoperative, perkutane Methode [The transjugular intrahepatic portosystemic stent-shunt. A new nonsurgical percutaneous method]. Radiologe. 1989;29(8):406-411. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources