

Prevalence and mortality of ceftazidime/avibactam-resistant KPC-producing Klebsiella pneumoniae bloodstream infections (2018-2022)
- PMID: 37985552
- PMCID: PMC10774640
- DOI: 10.1007/s10096-023-04712-8
Prevalence and mortality of ceftazidime/avibactam-resistant KPC-producing Klebsiella pneumoniae bloodstream infections (2018-2022)
Abstract
Introduction: Ceftazidime/avibactam-resistance in Klebsiella pneumoniae carbapenemase-producing Klebsiella pneumoniae (KPC-Kp) is a topic of great interest for epidemiological, diagnostic, and therapeutical reasons. However, data on its prevalence and burden on mortality in patients with bloodstream infection (BSI) are lacking. This study was aimed at identifying risk factors for mortality in patients suffering from ceftazidime/avibactam-resistant KPC-Kp BSI.
Methods: An observational retrospective study (January 2018-December 2022) was conducted at a tertiary hospital including all consecutive hospitalized adult patients with a ceftazidime/avibactam-resistant KPC-Kp BSI. Data on baseline clinical features, management, and admission outcomes were analyzed.
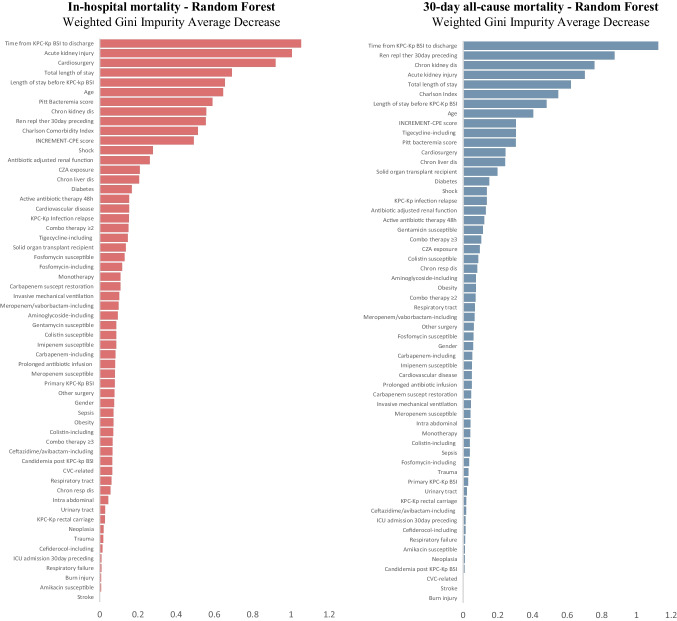
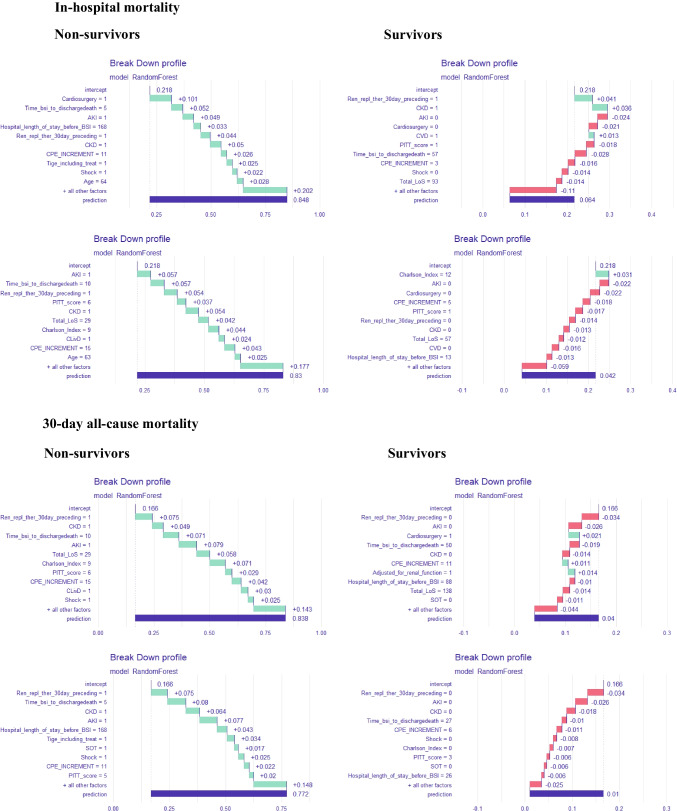
Results: Over the study period, among all the KPC-Kp BSI events recorded, 38 (10.5%) were caused by ceftazidime/avibactam-resistant KPC-Kp strains, 37 events being finally included. The ceftazidime/avibactam-resistant KPC-Kp strains revealed susceptibility restoration to at least one carbapenem in more than 60% of cases. In-hospital and 30-day all-cause mortality rates were 22% and 16.2%, respectively. Non-survivors suffered from more baseline comorbidities and experienced a more severe ceftazidime/avibactam-resistant KPC-Kp BSI presentation (i.e., both the Pitt Bacteremia and INCREMENT-CPE scores were significantly higher). Presenting with a higher Charlson Comorbidity Index, chronic kidney disease-KDIGO stage 3A or worse-having recently gone through renal replacement therapy, having suffered from an acute kidney injury following the ceftazidime/avibactam-resistant KPC-Kp BSI, and being admitted for cardiac surgery were the strongest predictors of mortality.
Conclusion: Ceftazidime/avibactam resistance in KPC-Kp BSI easily emerged in our highly KPC-Kp endemic area with remarkable mortality rates. Our findings might provide physicians possibly actionable information when managing patients with a ceftazidime/avibactam-resistant KPC-Kp BSI.
Keywords: Bloodstream infection; Ceftazidime/avibactam resistance; KPC; Klebsiella pneumoniae; Mortality; Sepsis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Iacchini S, Sabbatucci M, Gagliotti C, Rossolini GM, Moro ML, Iannazzo S, et al. Bloodstream infections due to carbapenemase-producing Enterobacteriaceae in Italy: results from nationwide surveillance, 2014 to 2017. Euro Surveill. 2019;24:1800159. doi: 10.2807/1560-7917.ES.2019.24.5.1800159. - DOI - PMC - PubMed
-
- Tumbarello M, Raffaelli F, Giannella M, Mantengoli E, Mularoni A, Venditti M, et al. Ceftazidime-avibactam use for Klebsiella pneumoniae carbapenemase-producing K. pneumoniae infections: a retrospective observational multicenter study. Clin Infect Dis. 2021;73:1664–76. doi: 10.1093/cid/ciab176. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
