

Differential activation of programmed cell death in patients with severe SARS-CoV-2 infection
- PMID: 37985756
- PMCID: PMC10662024
- DOI: 10.1038/s41420-023-01715-4
Differential activation of programmed cell death in patients with severe SARS-CoV-2 infection
Abstract
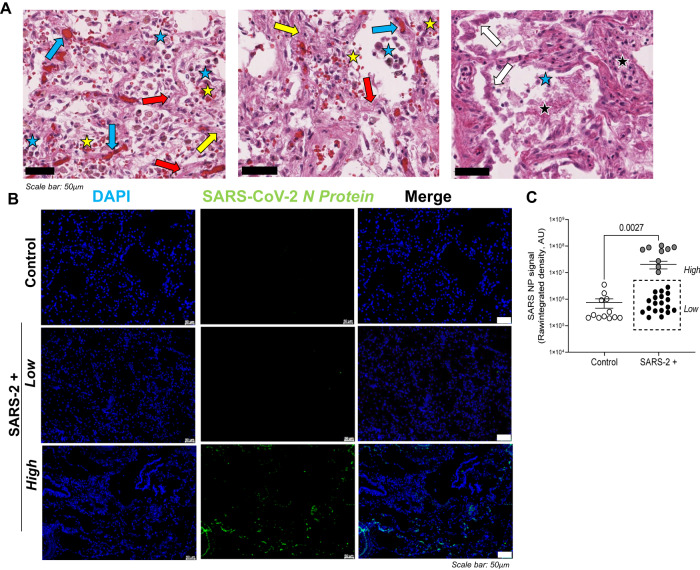
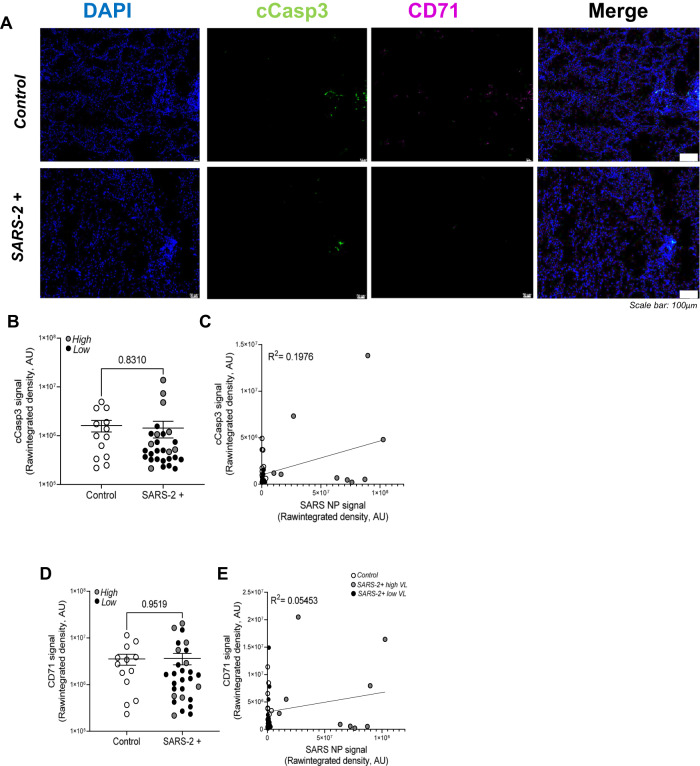
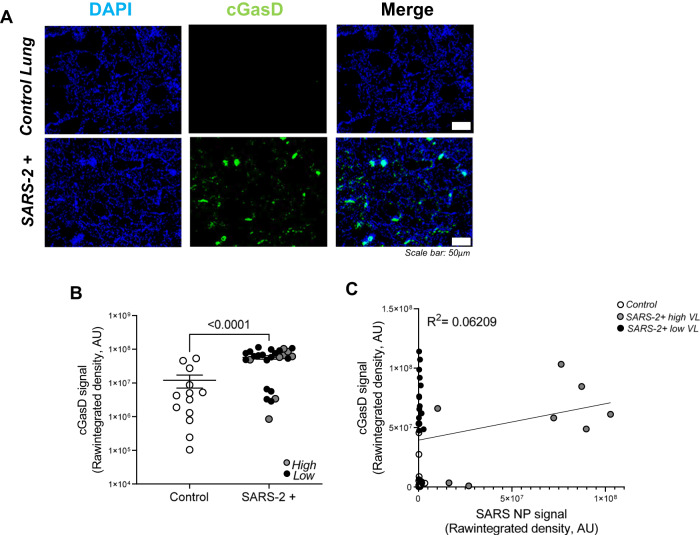
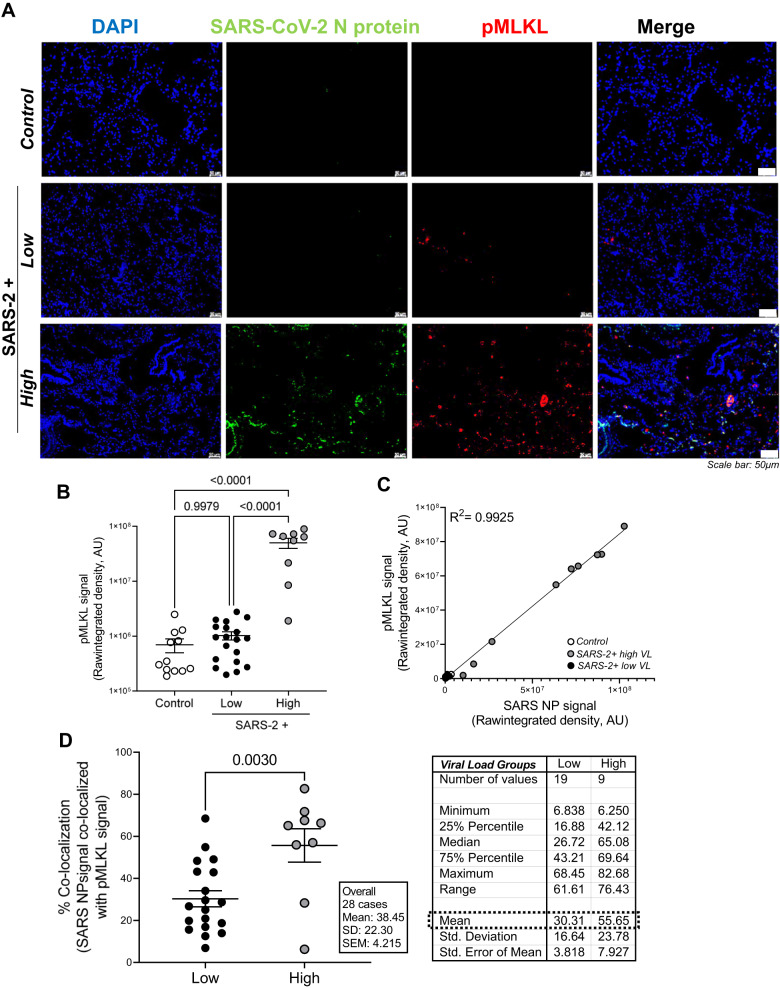
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes severe lower airway disease and death in a subset of patients. Knowledge on the relative contribution of programmed cell death (PCD) to lung pathology is limited to few human autopsy studies with small sample size/scope, in vitro cell culture, and experimental model systems. In this study, we sought to identify, localize, and quantify activation of apoptosis, ferroptosis, pyroptosis, and necroptosis in FFPE lung tissues from patients that died from severe SARS-CoV-2 infection (n = 28) relative to uninfected controls (n = 13). Immunofluorescence (IF) staining, whole-slide imaging, and Image J software was used to localize and quantify expression of SARS-CoV-2 nucleoprotein and the following PCD protein markers: cleaved Caspase-3, pMLKL, cleaved Gasdermin D, and CD71, respectively. IF showed differential activation of each PCD pathway in infected lungs and dichotomous staining for SARS-CoV-2 nucleoprotein enabling distinction between high (n = 9) vs low viral burden (n = 19). No differences were observed in apoptosis and ferroptosis in SARS-CoV-2 infected lungs relative to uninfected controls. However, both pyroptosis and necroptosis were significantly increased in SARS-CoV-2-infected lungs. Increased pyroptosis was observed in SARS-CoV-2 infected lungs, irrespective of viral burden, suggesting an inflammation-driven mechanism. In contrast, necroptosis exhibited a very strong positive correlation with viral burden (R2 = 0.9925), suggesting a direct SARS-CoV-2 mediated effect. These data indicate a possible novel mechanism for viral-mediated necroptosis and a potential role for both lytic programmed cell death pathways, necroptosis and pyroptosis, in mediating infection outcome.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
Differential Activation of Programmed Cell Death in Patients with Severe SARS-CoV-2 Infection.Res Sq [Preprint]. 2023 Jun 27:rs.3.rs-3059466. doi: 10.21203/rs.3.rs-3059466/v1. Res Sq. 2023. Update in: Cell Death Discov. 2023 Nov 20;9(1):420. doi: 10.1038/s41420-023-01715-4. PMID: 37461686 Free PMC article. Updated. Preprint.
Similar articles
-
Differential Activation of Programmed Cell Death in Patients with Severe SARS-CoV-2 Infection.Res Sq [Preprint]. 2023 Jun 27:rs.3.rs-3059466. doi: 10.21203/rs.3.rs-3059466/v1. Res Sq. 2023. Update in: Cell Death Discov. 2023 Nov 20;9(1):420. doi: 10.1038/s41420-023-01715-4. PMID: 37461686 Free PMC article. Updated. Preprint.
-
SARS-CoV-2 infection of polarized human airway epithelium induces necroptosis that causes airway epithelial barrier dysfunction.J Med Virol. 2023 Sep;95(9):e29076. doi: 10.1002/jmv.29076. J Med Virol. 2023. PMID: 37671751 Free PMC article.
-
Coronavirus Infection-Associated Cell Death Signaling and Potential Therapeutic Targets.Molecules. 2021 Dec 9;26(24):7459. doi: 10.3390/molecules26247459. Molecules. 2021. PMID: 34946543 Free PMC article. Review.
-
The Defenders of the Alveolus Succumb in COVID-19 Pneumonia to SARS-CoV-2 and Necroptosis, Pyroptosis, and PANoptosis.J Infect Dis. 2023 May 29;227(11):1245-1254. doi: 10.1093/infdis/jiad056. J Infect Dis. 2023. PMID: 36869698 Free PMC article.
-
PANoptosis in Viral Infection: The Missing Puzzle Piece in the Cell Death Field.J Mol Biol. 2022 Feb 28;434(4):167249. doi: 10.1016/j.jmb.2021.167249. Epub 2021 Sep 16. J Mol Biol. 2022. PMID: 34537233 Free PMC article. Review.
Cited by
-
TRIM7 ubiquitinates SARS-CoV-2 membrane protein to limit apoptosis and viral replication.bioRxiv [Preprint]. 2024 Jun 17:2024.06.17.599107. doi: 10.1101/2024.06.17.599107. bioRxiv. 2024. Update in: Nat Commun. 2024 Nov 30;15(1):10438. doi: 10.1038/s41467-024-54762-5. PMID: 38948778 Free PMC article. Updated. Preprint.
-
TRIM7 ubiquitinates SARS-CoV-2 membrane protein to limit apoptosis and viral replication.Nat Commun. 2024 Nov 30;15(1):10438. doi: 10.1038/s41467-024-54762-5. Nat Commun. 2024. PMID: 39616206 Free PMC article.
-
The role of programmed cell death in organ dysfunction induced by opportunistic pathogens.Crit Care. 2025 Jan 24;29(1):43. doi: 10.1186/s13054-025-05278-x. Crit Care. 2025. PMID: 39856779 Free PMC article. Review.
-
The Anti-Oxidative, Anti-Inflammatory, Anti-Apoptotic, and Anti-Necroptotic Role of Zinc in COVID-19 and Sepsis.Antioxidants (Basel). 2023 Oct 31;12(11):1942. doi: 10.3390/antiox12111942. Antioxidants (Basel). 2023. PMID: 38001795 Free PMC article. Review.
-
A glimpse into viral warfare: decoding the intriguing role of highly pathogenic coronavirus proteins in apoptosis regulation.J Biomed Sci. 2024 Jul 13;31(1):70. doi: 10.1186/s12929-024-01062-1. J Biomed Sci. 2024. PMID: 39003473 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
