

The immunoregulatory roles of non-haematopoietic cells in the kidney
- PMID: 37985868
- PMCID: PMC11005998
- DOI: 10.1038/s41581-023-00786-x
The immunoregulatory roles of non-haematopoietic cells in the kidney
Erratum in
-
Author Correction: The immunoregulatory roles of non-haematopoietic cells in the kidney.Nat Rev Nephrol. 2024 Jan;20(1):70. doi: 10.1038/s41581-023-00793-y. Nat Rev Nephrol. 2024. PMID: 37996613 Free PMC article. No abstract available.
Abstract
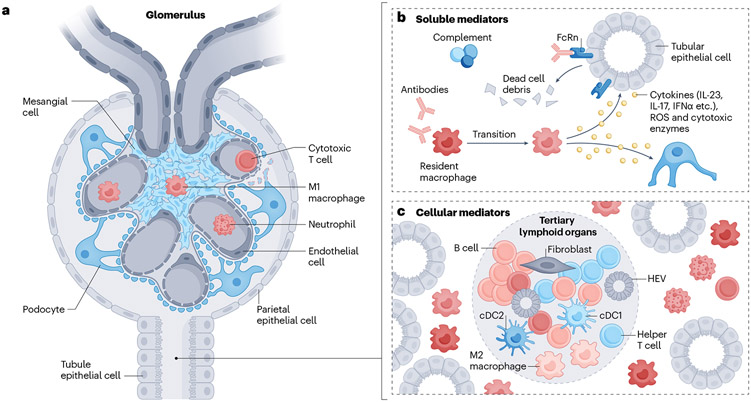
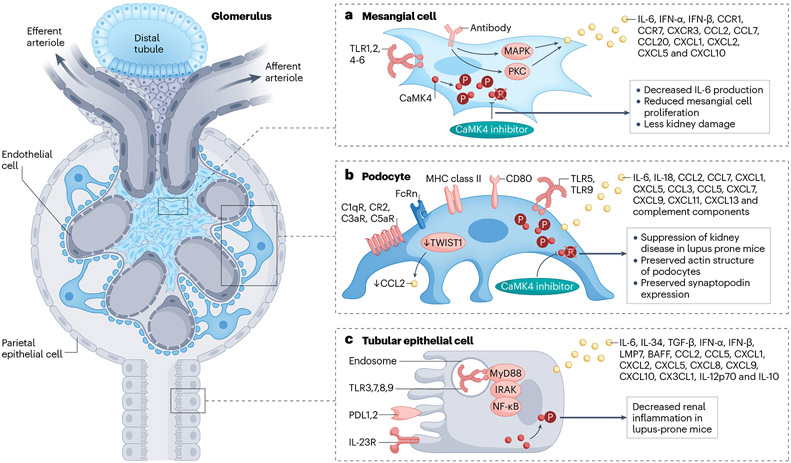
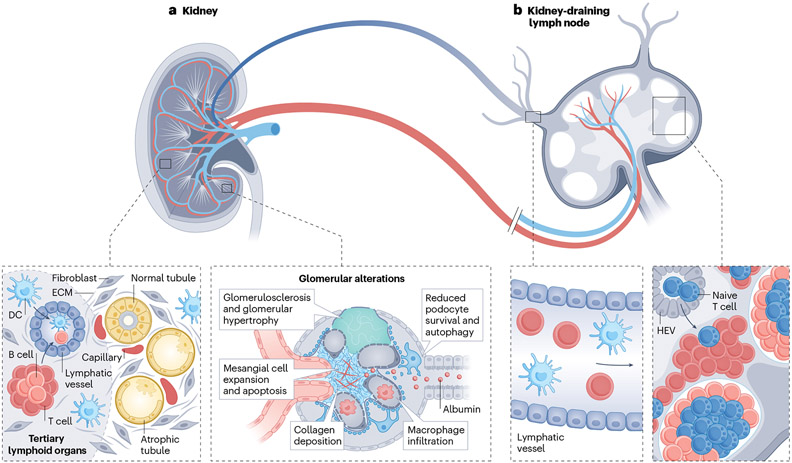
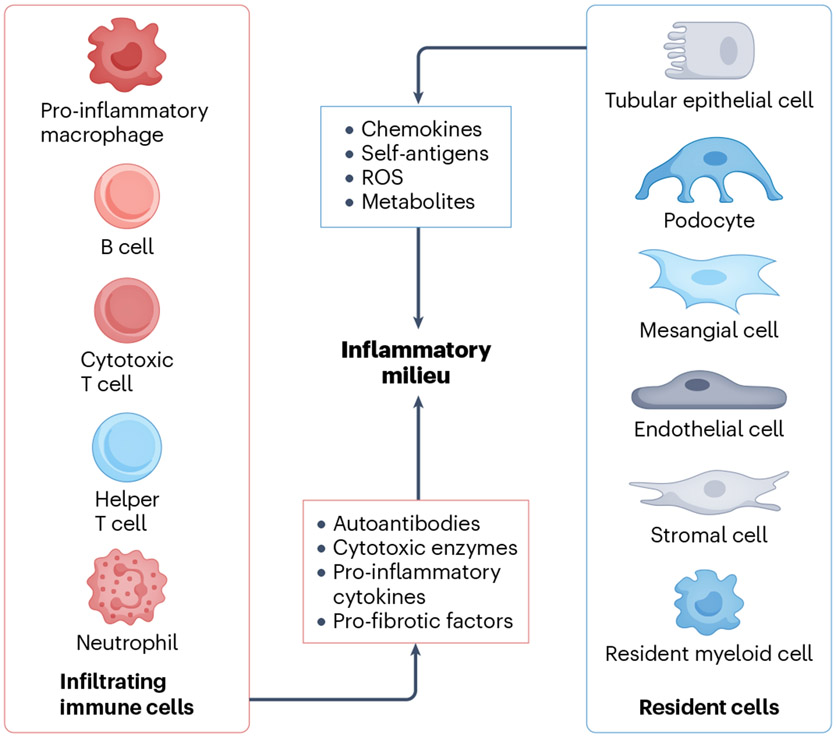
The deposition of immune complexes, activation of complement and infiltration of the kidney by cells of the adaptive and innate immune systems have long been considered responsible for the induction of kidney damage in autoimmune, alloimmune and other inflammatory kidney diseases. However, emerging findings have highlighted the contribution of resident immune cells and of immune molecules expressed by kidney-resident parenchymal cells to disease processes. Several types of kidney parenchymal cells seem to express a variety of immune molecules with a distinct topographic distribution, which may reflect the exposure of these cells to different pathogenic threats or microenvironments. A growing body of literature suggests that these cells can stimulate the infiltration of immune cells that provide protection against infections or contribute to inflammation - a process that is also regulated by draining kidney lymph nodes. Moreover, components of the immune system, such as autoantibodies, cytokines and immune cells, can influence the metabolic profile of kidney parenchymal cells in the kidney, highlighting the importance of crosstalk in pathogenic processes. The development of targeted nanomedicine approaches that modulate the immune response or control inflammation and damage directly within the kidney has the potential to eliminate the need for systemically acting drugs.
© 2023. Springer Nature Limited.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
