

The optimal dose of mobilisation therapy in the ICU: a prospective cohort study
- PMID: 37986100
- PMCID: PMC10658796
- DOI: 10.1186/s40560-023-00703-1
The optimal dose of mobilisation therapy in the ICU: a prospective cohort study
Abstract
Background: This study aimed to assess the impact of duration of early mobilisation on survivors of critical illness. The hypothesis was that interventions lasting over 40 min, as per the German guideline, positively affect the functional status at ICU discharge.
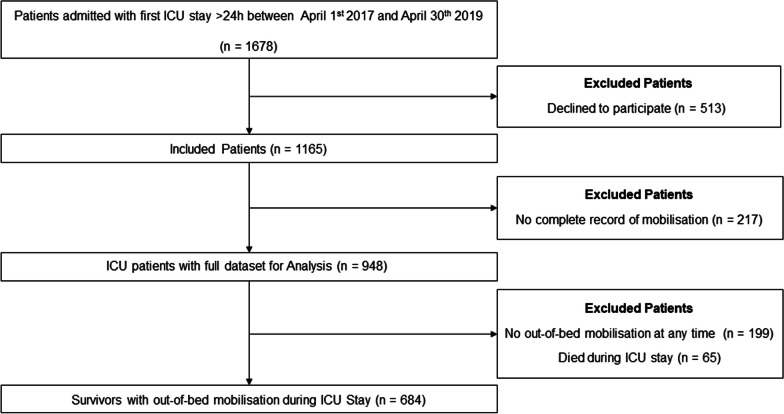
Methods: Prospective single-centre cohort study conducted in two ICUs in Germany. In 684 critically ill patients surviving an ICU stay > 24 h, out-of-bed mobilisation of more than 40 min was evaluated.
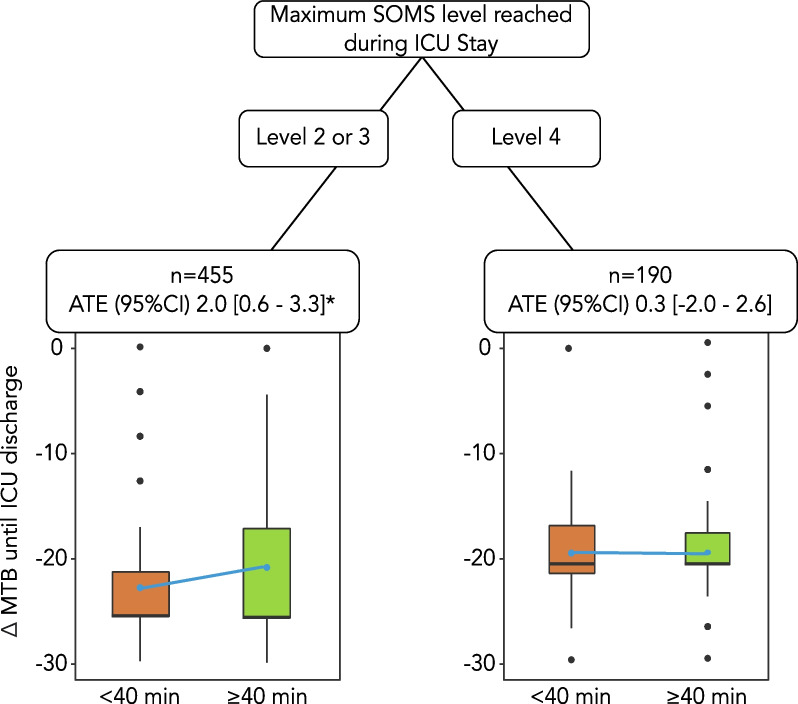
Results: Daily mobilisation ≥ 40 min was identified as an independent predictor of an improved functional status upon ICU discharge. This effect on the primary outcome measure, change of Mobility-Barthel until ICU discharge, was observed in three different models for baseline patient characteristics (average treatment effect (ATE), all three models p < 0.001). When mobilisation parameters like level of mobilisation, were included in the analysis, the average treatment effect disappeared [ATE 1.0 (95% CI - 0.4 to 2.4), p = 0.16].
Conclusions: A mobilisation duration of more than 40 min positively impacts functional outcomes at ICU discharge. However, the maximum level achieved during ICU stay was the most crucial factor regarding adequate dosage, as higher duration did not show an additional benefit in patients with already high mobilisation levels.
Trial registration: Prospective Registry of Mobilization-, Routine- and Outcome Data of Intensive Care Patients (MOBDB), NCT03666286. Registered 11 September 2018-retrospectively registered, https://classic.
Clinicaltrials: gov/ct2/show/NCT03666286 .
Keywords: Early mobilisation; Functional status; ICU; Mobilisation; Physical therapy modalities.
© 2023. The Author(s).
Conflict of interest statement
SJS received grants and non-financial support from Reactive Robotics GmbH (Munich, Germany), ASP GmbH (Attendorn, Germany), STIMIT AG (Biel, Switzerland), ESICM (Geneva, Switzerland), grants, personal fees, and non-financial support from Fresenius Kabi Deutschland GmbH (Bad Homburg, Germany), grants from the Innovationsfond of The Federal Joint Committee (G-BA), personal fees from Springer Verlag GmbH (Vienna, Austria) for educational purposes and Advanz Pharma GmbH (Bielefeld, Germany), non-financial support from national and international societies (and their congress organisers) in the field of anesthesiology and intensive care medicine, outside the submitted work. Dr. Schaller holds stocks in small amounts from Alphabet Inc., Bayer AG, and Siemens AG; these holdings have not affected any decisions regarding his research or this study.
Figures
References
-
- Spies CD, Krampe H, Paul N, Denke C, Kiselev J, Piper SK, et al. Instruments to measure outcomes of post-intensive care syndrome in outpatient care settings—results of an expert consensus and feasibility field test. J Intensive Care Soc. 2021;22(2):159–174. doi: 10.1177/1751143720923597. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
