

Diabetes mellitus affects the treatment outcomes of drug-resistant tuberculosis: a systematic review and meta-analysis
- PMID: 37986146
- PMCID: PMC10662654
- DOI: 10.1186/s12879-023-08765-0
Diabetes mellitus affects the treatment outcomes of drug-resistant tuberculosis: a systematic review and meta-analysis
Abstract
Background: Both tuberculosis (TB) and diabetes mellitus (DM) are major public health problems threatening global health. TB patients with DM have a higher bacterial burden and affect the absorption and metabolism for anti-TB drugs. Drug-resistant TB (DR-TB) with DM make control TB more difficult.
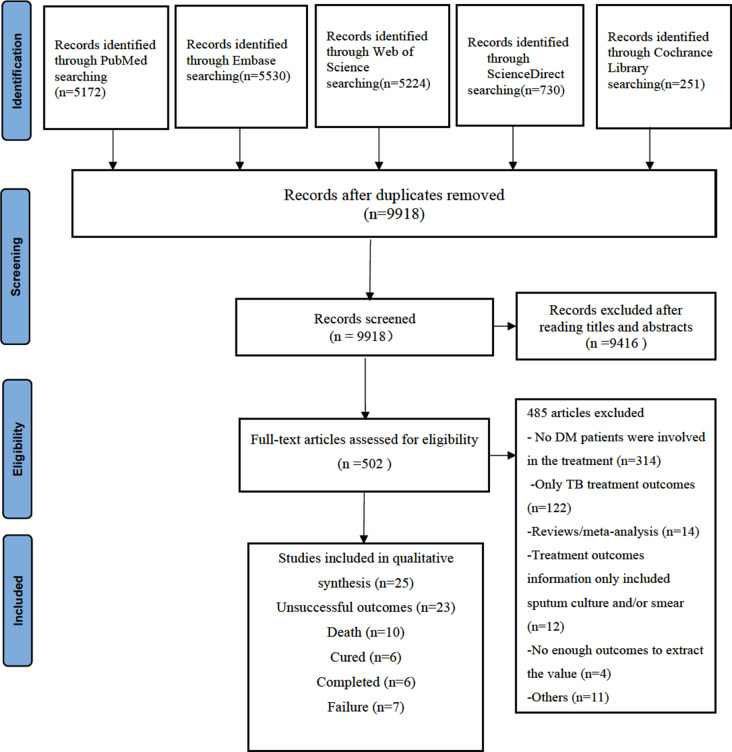
Methods: This study was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guideline. We searched PubMed, Excerpta Medica Database (EMBASE), Web of Science, ScienceDirect and Cochrance Library for literature published in English until July 2022. Papers were limited to those reporting the association between DM and treatment outcomes among DR-TB and multidrug-resistant TB (MDR-TB) patients. The strength of association was presented as odds ratios (ORs) and their 95% confidence intervals (CIs) using the fixed-effects or random-effects models. This study was registered with PROSPERO, number CRD: 42,022,350,214.
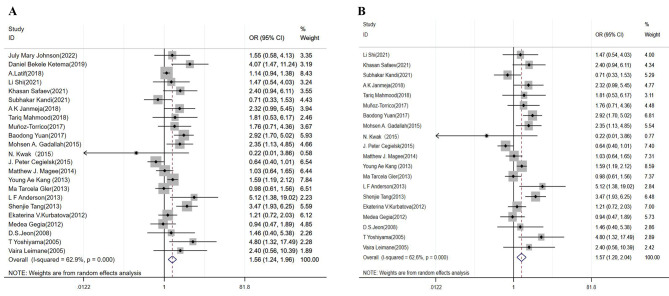
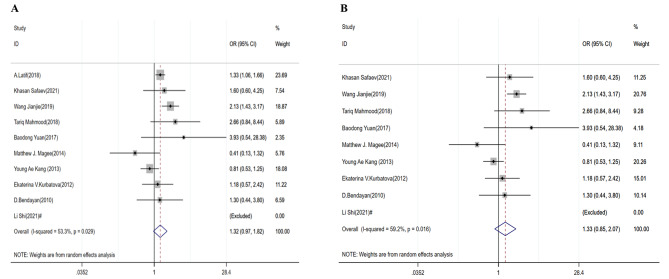
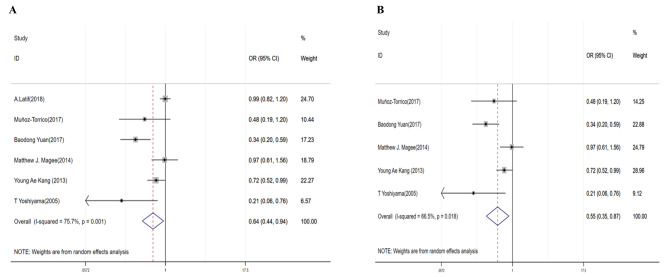
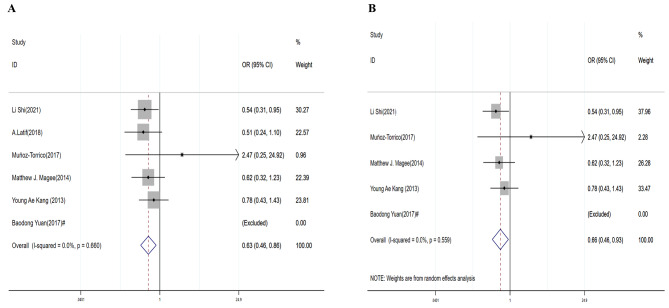
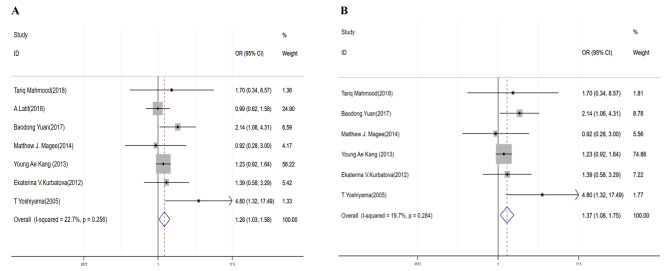
Results: A total of twenty-five studies involving 16,905 DR-TB participants were included in the meta-analysis, of which 10,124 (59.89%) participants were MDR-TB patients, and 1,952 (11.54%) had DM history. In DR-TB patients, the pooled OR was 1.56 (95% CI: 1.24-1.96) for unsuccessful outcomes, 0.64 (95% CI: 0.44-0.94) for cured treatment outcomes, 0.63 (95% CI: 0.46-0.86) for completed treatment outcomes, and 1.28 (95% CI: 1.03-1.58) for treatment failure. Among MDR-TB patients, the pooled OR was 1.57 (95% CI: 1.20-2.04) for unsuccessful treatment outcomes, 0.55 (95% CI: 0.35-0.87) for cured treatment outcomes, 0.66 (95% CI: 0.46-0.93) for treatment completed treatment outcomes and 1.37 (95% CI: 1.08-1.75) for treatment failure.
Conclusion: DM is a risk factor for adverse outcomes of DR-TB or MDR-TB patients. Controlling hyperglycemia may contribute to the favorite prognosis of TB. Our findings support the importance for diagnosing DM in DR-TB /MDR-TB, and it is needed to control glucose and therapeutic monitoring during the treatment of DR-TB /MDR-TB patients.
Keywords: Diabetes mellitus; Drug-resistant tuberculosis; Multidrug-resistant tuberculosis; Treatment outcomes.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Association between diabetes mellitus and multi-drug-resistant tuberculosis: evidence from a systematic review and meta-analysis.Syst Rev. 2018 Oct 15;7(1):161. doi: 10.1186/s13643-018-0828-0. Syst Rev. 2018. PMID: 30322409 Free PMC article.
-
The effect size of type 2 diabetes mellitus on tuberculosis drug resistance and adverse treatment outcomes.Tuberculosis (Edinb). 2017 Mar;103:83-91. doi: 10.1016/j.tube.2017.01.006. Epub 2017 Jan 24. Tuberculosis (Edinb). 2017. PMID: 28237037
-
Risk Factors for Multidrug-resistant Tuberculosis.Acta Med Indones. 2018 Jan;50(1):1-2. Acta Med Indones. 2018. PMID: 29686169
-
Diabetes mellitus and the risk of multidrug resistant tuberculosis: a meta-analysis.Sci Rep. 2017 Apr 24;7(1):1090. doi: 10.1038/s41598-017-01213-5. Sci Rep. 2017. PMID: 28439071 Free PMC article.
-
HIV infection and multidrug resistant tuberculosis: a systematic review and meta-analysis.BMC Infect Dis. 2021 Jan 11;21(1):51. doi: 10.1186/s12879-020-05749-2. BMC Infect Dis. 2021. PMID: 33430786 Free PMC article.
Cited by
-
Role of therapeutic drug monitoring in the treatment of multi-drug resistant tuberculosis.J Clin Tuberc Other Mycobact Dis. 2024 Apr 24;36:100444. doi: 10.1016/j.jctube.2024.100444. eCollection 2024 Aug. J Clin Tuberc Other Mycobact Dis. 2024. PMID: 38708036 Free PMC article.
-
Multidrug-resistant tuberculosis.Nat Rev Dis Primers. 2024 Mar 24;10(1):22. doi: 10.1038/s41572-024-00504-2. Nat Rev Dis Primers. 2024. PMID: 38523140 Review.
-
High Rates of Mortality During Drug-Resistant Tuberculosis Treatment Among Individuals With Diabetes Mellitus and Low Body Mass Index.Open Forum Infect Dis. 2025 Jun 25;12(7):ofaf344. doi: 10.1093/ofid/ofaf344. eCollection 2025 Jul. Open Forum Infect Dis. 2025. PMID: 40599491 Free PMC article.
-
Optimizing Drug-Resistant Tuberculosis Treatment Outcomes in a High HIV-Burden Setting: A Study of Sputum Conversion and Regimen Efficacy in Rural South Africa.Pathogens. 2025 Apr 30;14(5):441. doi: 10.3390/pathogens14050441. Pathogens. 2025. PMID: 40430760 Free PMC article.
-
Hyperglycemic milieu impairs Vγ9Vδ2 T cell functions in tuberculosis patients and prolongs M.tb negative conversion time.iScience. 2024 Dec 26;28(1):111692. doi: 10.1016/j.isci.2024.111692. eCollection 2025 Jan 17. iScience. 2024. PMID: 39886461 Free PMC article.
References
-
- Lakoh S, Jiba DF, Adekanmbi O, Poveda E, Sahr F, Deen GF, Foray LM, Gashau W, Hoffmann CJ, Salata RA, et al. Diagnosis and treatment outcomes of adult Tuberculosis in an urban setting with high HIV prevalence in Sierra Leone: a retrospective study. Int J Infect Dis. 2020;96:112–8. doi: 10.1016/j.ijid.2020.04.038. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
