

This is a preprint.
Cost-effectiveness of broadly neutralizing antibodies for infant HIV prophylaxis in settings with high HIV burdens: a simulation modeling study
- PMID: 37986879
- PMCID: PMC10659508
- DOI: 10.1101/2023.11.06.23298184
Cost-effectiveness of broadly neutralizing antibodies for infant HIV prophylaxis in settings with high HIV burdens: a simulation modeling study
Update in
-
Cost-effectiveness of broadly neutralizing antibodies for HIV prophylaxis for infants born in settings with high HIV burdens.PLoS One. 2025 Mar 19;20(3):e0318940. doi: 10.1371/journal.pone.0318940. eCollection 2025. PLoS One. 2025. PMID: 40106399 Free PMC article.
Abstract
Introduction: Approximately 130 000 infants acquire HIV annually despite global maternal antiretroviral therapy scale-up. We evaluated the potential clinical impact and cost-effectiveness of offering long-acting, anti-HIV broadly neutralizing antibody (bNAb) prophylaxis to infants in three distinct settings.
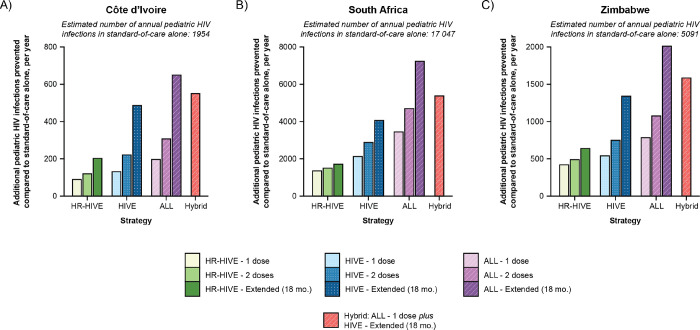
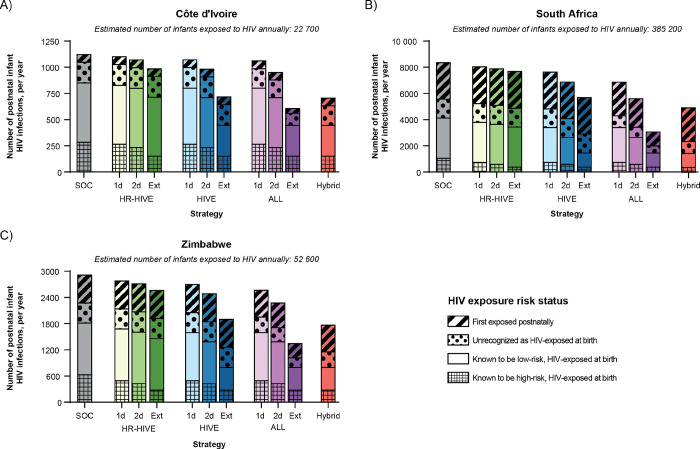
Methods: We simulated infants in Côte d'Ivoire, South Africa, and Zimbabwe using the Cost-Effectiveness of Preventing AIDS Complications-Pediatric (CEPAC-P) model. We modeled strategies offering a three-bNAb combination in addition to WHO-recommended standard-of-care oral prophylaxis to infants: a) with known, WHO-defined high-risk HIV exposure at birth (HR-HIVE); b) with known HIV exposure at birth (HIVE); or c) with or without known HIV exposure (ALL). Modeled infants received 1-dose, 2-doses, or Extended (every 3 months through 18 months) bNAb dosing. Base case model inputs included 70% bNAb efficacy (sensitivity analysis range: 10-100%), 3-month efficacy duration/dosing interval (1-6 months), and $20/dose cost ($5-$100/dose). Outcomes included pediatric HIV infections, life expectancy, lifetime HIV-related costs, and incremental cost-effectiveness ratios (ICERs, in US$/year-of-life-saved [YLS], assuming a ≤50% GDP per capita cost-effectiveness threshold).
Results: The base case model projects that bNAb strategies targeting HIVE and ALL infants would prevent 7-26% and 10-42% additional pediatric HIV infections, respectively, compared to standard-of-care alone, ranging by dosing approach. HIVE-Extended would be cost-effective (cost-saving compared to standard-of-care) in Côte d'Ivoire and Zimbabwe; ALL-Extended would be cost-effective in South Africa (ICER: $882/YLS). BNAb strategies targeting HR-HIVE infants would result in greater lifetime costs and smaller life expectancy gains than HIVE-Extended. Throughout most bNAb efficacies and costs evaluated in sensitivity analyses, targeting HIVE infants would be cost-effective in Côte d'Ivoire and Zimbabwe, and targeting ALL infants would be cost-effective in South Africa.
Discussion: Adding long-acting bNAbs to current standard-of-care prophylaxis would be cost-effective, assuming plausible efficacies and costs. The cost-effective target population would vary by setting, largely driven by maternal antenatal HIV prevalence and postpartum incidence.
Conflict of interest statement
Conflicts of Interest: SP is a consultant for Merck, Moderna, Pfizer, Dynavax, Hoopika, and GSK, and has a sponsored research program with Moderna and Merck in the area of cytomegalovirus (CMV) vaccines. AG is a co-PI on COVID-vaccine studies funded through the SAMRC by the HIV vaccine trials network, EDCTP, ANRS, ImmunityBio, Janssen, and Moderna. AB and EJF receive funding from IMPAACT and AB receives funding from Unitaid for trials evaluating non-bNAb approaches to maternal-infant HIV prophylaxis. CKC participated in a RSV advisory board for Sanofi and previously received grants from Gilead, paid to her University, for clinical research. SM, KC, PEF, DS, and VMK are employed by IAVI, a non-profit organization that is pursuing the development of a combination anti-HIV bNAb product. No other authors report conflicts of interest.
Figures

References
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS). The path that ends AIDS: UNAIDS Global AIDS Update 2023. Accessed September 17, 2023. https://www.unaids.org/sites/default/files/media_asset/2023-unaids-globa...
-
- Joint United Nations Programme on HIV/AIDS. 2021. UNAIDS Global AIDS Update – Confronting inequalities – Lessons for pandemic responses from 40 years of AIDS. Accessed October 6, 2022. https://www.unaids.org/en/resources/documents/2021/2021-global-aids-update
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources