

Application of Precision Medicine Concepts in Ambulatory Antibiotic Management of Acute Pyelonephritis
- PMID: 37987379
- PMCID: PMC10661281
- DOI: 10.3390/pharmacy11060169
Application of Precision Medicine Concepts in Ambulatory Antibiotic Management of Acute Pyelonephritis
Abstract
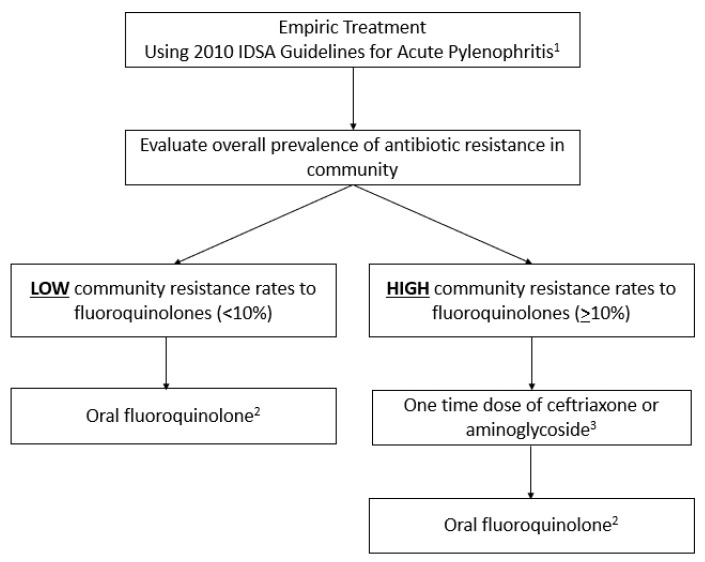
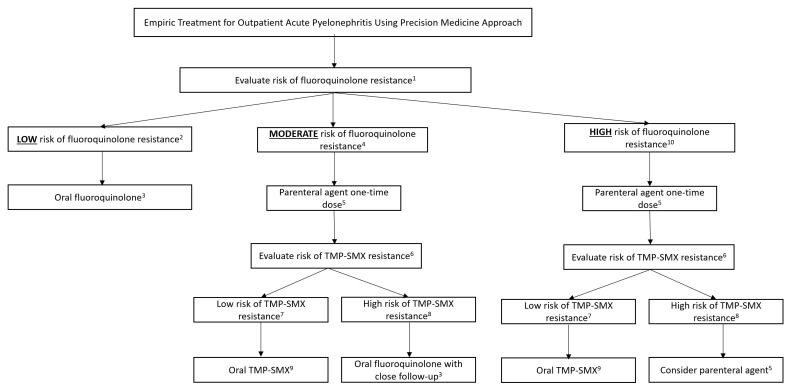
Acute pyelonephritis (APN) is a relatively common community-acquired infection, particularly in women. The early appropriate antibiotic treatment of this potentially life-threatening infection is associated with improved outcomes. The international management guidelines for complicated urinary tract infections and APN recommend using oral antibiotics with <10% resistance among urinary pathogens. However, increasing antibiotic resistance rates among Escherichia coli and other Enterobacterales to fluoroquinolones, trimethoprim-sulfamethoxazole (TMP-SMX), and beta-lactams has left patients without reliable oral antibiotic treatment options for APN. This narrative review proposes using precision medicine concepts to improve empirical antibiotic therapy for APN in ambulatory settings. Whereas resistance rates to a particular antibiotic class may exceed 10% at the population-based level, the predicted antibiotic resistance rates based on patient-specific risk factors fall under 10% in many patients with APN on the individual level. The utilization of clinical tools for the prediction of fluoroquinolones, TMP-SMX, and third-generation cephalosporin resistance improves the ambulatory antibiotic management of APN. It may also reduce the need to switch antibiotic therapy later based on the in vitro antibiotic susceptibility testing results of bacterial isolates in urinary cultures. This approach may mitigate the burden of increasing antibiotic resistance in the community by ensuring that the initial antibiotic prescribed has the highest likelihood of treating APN appropriately.
Keywords: acute pyelonephritis; antibiotic resistance; outpatient antibiotic stewardship; precision medicine; transitions of care.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Talan D.A., Takhar S.S., Krishnadasan A., Abrahamian F.M., Mower W.R., Moran G.J., EMERG Ency ID Net Study Group Fluoroquinolone-Resistant and Extended-Spectrum B-Lactamase-Producing Escherichia coli Infections in Patients with Pyelonephritis, United States. Emerg. Infect. Dis. 2016;22:1594–1603. doi: 10.3201/eid2209.160148. - DOI - PMC - PubMed
-
- Gupta K., Hooton T.M., Naber K.G., Wullt B., Colgan R., Miller L.G., Moran G.J., Nicolle L.E., Raz R., Schaeffer A.J., et al. International Clinical Practice Guideline for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011;52:103–120. doi: 10.1093/cid/ciq257. - DOI - PubMed
-
- Zhanel G.G., Hisanaga T.L., Laing N.M., DeCorby M.R., Nichol K.A., Weshnoweski B., Johnson J., Noreddin A., Low D.E., Karlowsky J.A., et al. Antibiotic resistance in Escherichia coli outpatient urinary isolates: Final results from the North American Urinary Tract Infection Collaborative Alliance (NAUTICA) Int. J. Antimicrob. Agents. 2006;6:468–475. doi: 10.1016/j.ijantimicag.2006.02.009. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
