

The effect of higher or lower mean arterial pressure on kidney function after cardiac arrest: a post hoc analysis of the COMACARE and NEUROPROTECT trials
- PMID: 37987871
- PMCID: PMC10663425
- DOI: 10.1186/s13613-023-01210-0
The effect of higher or lower mean arterial pressure on kidney function after cardiac arrest: a post hoc analysis of the COMACARE and NEUROPROTECT trials
Abstract
Background: We aimed to study the incidence of acute kidney injury (AKI) in out-of-hospital cardiac arrest (OHCA) patients treated according to low-normal or high-normal mean arterial pressure (MAP) targets.
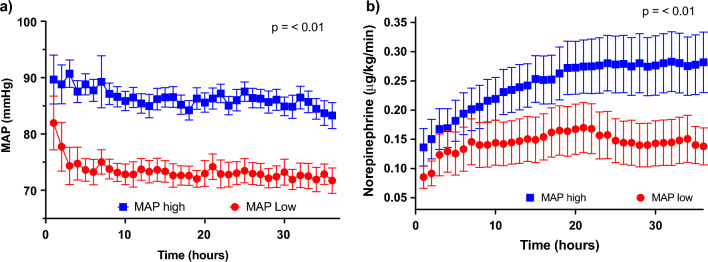
Methods: A post hoc analysis of the COMACARE (NCT02698917) and Neuroprotect (NCT02541591) trials that randomized patients to lower or higher targets for the first 36 h of intensive care. Kidney function was defined using the Kidney Disease Improving Global Outcome (KDIGO) classification. We used Cox regression analysis to identify factors associated with AKI after OHCA.
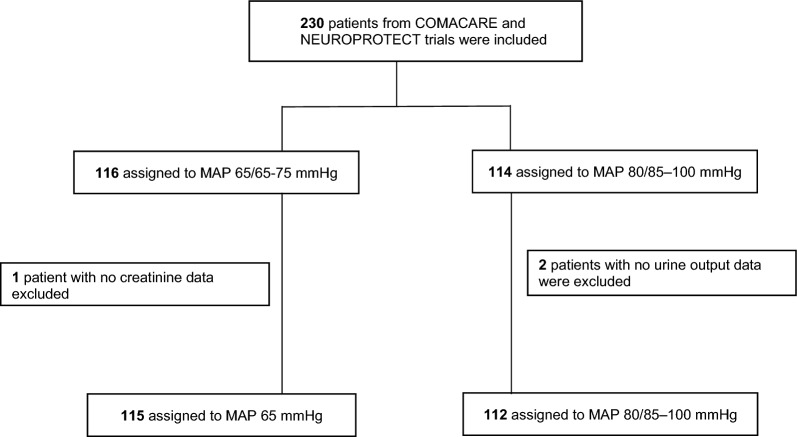
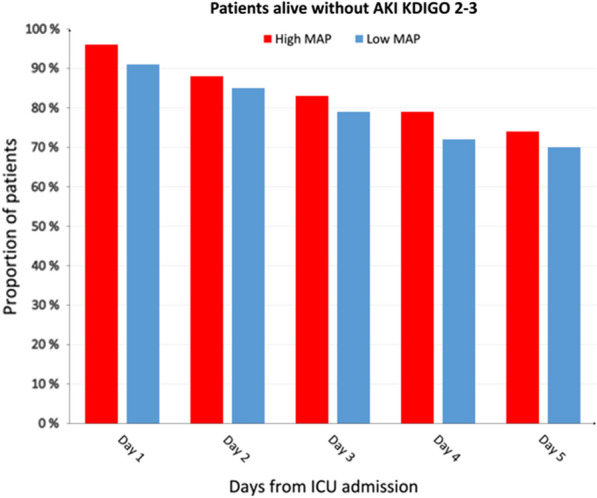
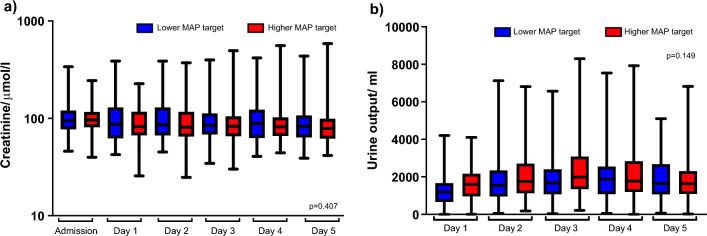
Results: A total of 227 patients were included: 115 in the high-normal MAP group and 112 in the low-normal MAP group. Eighty-six (38%) patients developed AKI during the first five days; 40 in the high-normal MAP group and 46 in the low-normal MAP group (p = 0.51). The median creatinine and daily urine output were 85 μmol/l and 1730 mL/day in the high-normal MAP group and 87 μmol/l and 1560 mL/day in the low-normal MAP group. In a Cox regression model, independent AKI predictors were no bystander cardiopulmonary resuscitation (p < 0.01), non-shockable rhythm (p < 0.01), chronic hypertension (p = 0.03), and time to the return of spontaneous circulation (p < 0.01), whereas MAP target was not an independent predictor (p = 0.29).
Conclusion: Any AKI occurred in four out of ten OHCA patients. We found no difference in the incidence of AKI between the patients treated with lower and those treated with higher MAP after CA. Higher age, non-shockable initial rhythm, and longer time to ROSC were associated with shorter time to AKI.
Clinical trial registration: COMACARE (NCT02698917), NEUROPROTECT (NCT02541591).
Keywords: Acute kidney injury; Kidney Disease Improving Global Outcomes; Out-of-hospital cardiac arrest.
© 2023. The Author(s).
Conflict of interest statement
Markus Skrifvars has received speaker’s fees from BARD Medical (Ireland).
Figures
References
-
- Martensson J, Bellomo R. Acute kidney injury after cardiac arrest: an unappreciated complication. Minerva Anestesiol. 2016;82:929–931. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
