

Lower muscle mitochondrial energetics is associated with greater phenotypic frailty in older women and men: the Study of Muscle, Mobility and Aging
- PMID: 37987886
- PMCID: PMC10828481
- DOI: 10.1007/s11357-023-01002-1
Lower muscle mitochondrial energetics is associated with greater phenotypic frailty in older women and men: the Study of Muscle, Mobility and Aging
Abstract
Background: Phenotypic frailty syndrome identifies older adults at greater risk for adverse health outcomes. Despite the critical role of mitochondria in maintaining cellular function, including energy production, the associations between muscle mitochondrial energetics and frailty have not been widely explored in a large, well-phenotyped, older population.
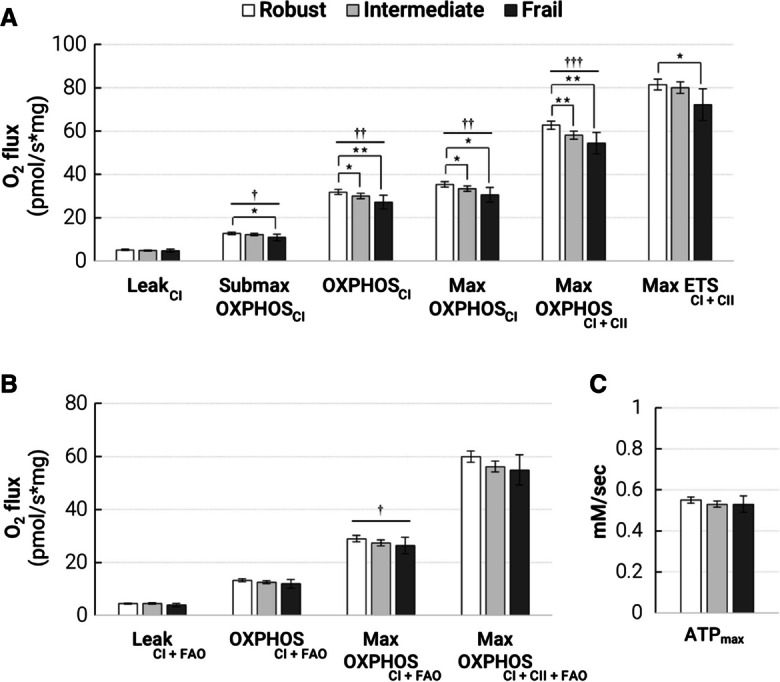
Methods: The Study of Muscle, Mobility and Aging (SOMMA) assessed muscle energetics in older adults (N = 879, mean age = 76.3 years, 59.2% women). 31Phosporous magnetic resonance spectroscopy measured maximal production of adenosine triphosphate (ATPmax) in vivo, while ex vivo high-resolution respirometry of permeabilized muscle fibers from the vastus lateralis measured maximal oxygen consumption supported by fatty acids and complex I- and II-linked carbohydrates (e.g., Max OXPHOSCI+CII). Five frailty criteria, shrinking, weakness, exhaustion, slowness, and low activity, were used to classify participants as robust (0, N = 397), intermediate (1-2, N = 410), or frail (≥ 3, N = 66). We estimated the proportional odds ratio (POR) for greater frailty, adjusted for multiple potential confounders.
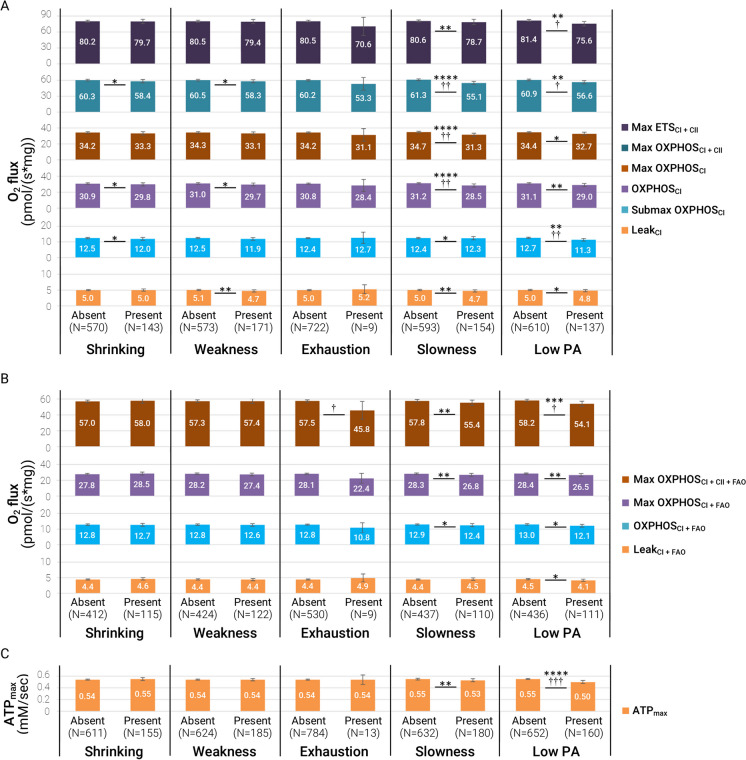
Results: One-SD decrements of most respirometry measures (e.g., Max OXPHOSCI+CII, adjusted POR = 1.5, 95%CI [1.2,1.8], p = 0.0001) were significantly associated with greater frailty classification. The associations of ATPmax with frailty were weaker than those between Max OXPHOSCI+CII and frailty. Muscle energetics was most strongly associated with slowness and low physical activity components.
Conclusions: Our data suggest that deficits in muscle mitochondrial energetics may be a biological driver of frailty in older adults. On the other hand, we did observe differential relationships between measures of muscle mitochondrial energetics and the individual components of frailty.
Keywords: Aging; Mitochondria; Muscle energetics; Phenotypic frailty.
© 2023. The Author(s), under exclusive licence to American Aging Association.
Conflict of interest statement
SRC and PMCa are consultants to Bioage Labs. PMCa is a consultant to and owns stock in MyoCorps. All other authors report no potential competing or conflicts of interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
- R01 AG058883/AG/NIA NIH HHS/United States
- R03 AG067937 and K76 AG074903/AG/NIA NIH HHS/United States
- P01 AG001751/AG/NIA NIH HHS/United States
- R01AG059416/AG/NIA NIH HHS/United States
- R03 AG067937/AG/NIA NIH HHS/United States
- P30AG021332/AG/NIA NIH HHS/United States
- P30 AG044281/AG/NIA NIH HHS/United States
- R01AG060153/AG/NIA NIH HHS/United States
- K76 AG074903/AG/NIA NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- P30AG024827/AG/NIA NIH HHS/United States
- UL1TR001420/TR/NCATS NIH HHS/United States
- R01 AG059416/AG/NIA NIH HHS/United States
- P30 AG024827/AG/NIA NIH HHS/United States
- P30 AG021332/AG/NIA NIH HHS/United States
- R01 AG060153/AG/NIA NIH HHS/United States
