

Developing a diagnostic framework for patients presenting with Exercise Induced Leg Pain (EILP): a scoping review
- PMID: 37990284
- PMCID: PMC10662794
- DOI: 10.1186/s13047-023-00680-6
Developing a diagnostic framework for patients presenting with Exercise Induced Leg Pain (EILP): a scoping review
Abstract
Background: Numerous conditions are grouped under the generic term exercise-induced leg pain (EILP), yet clear diagnostic guidelines are lacking. This scoping review was conducted to clarify the definition and diagnostic criteria of nine commonly occurring EILP conditions.
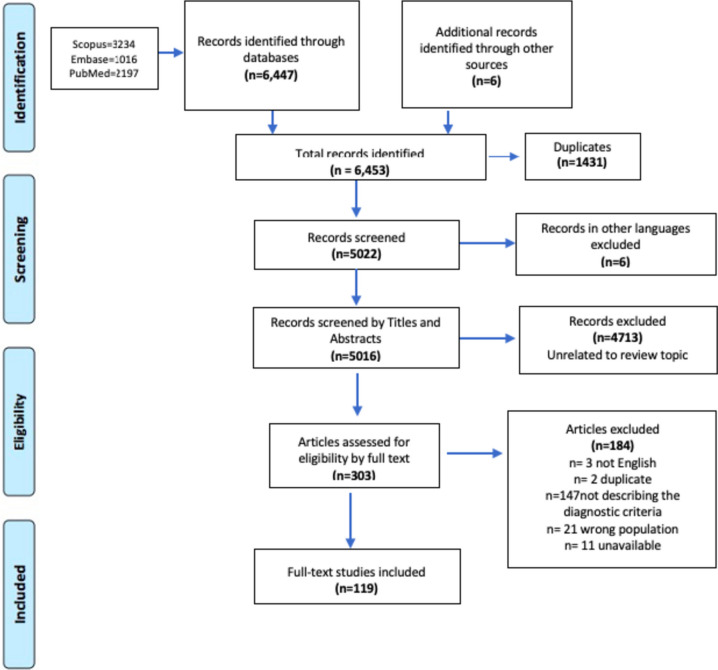
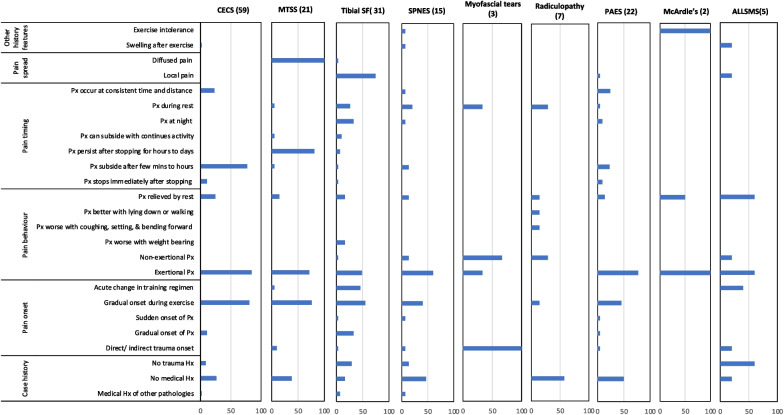
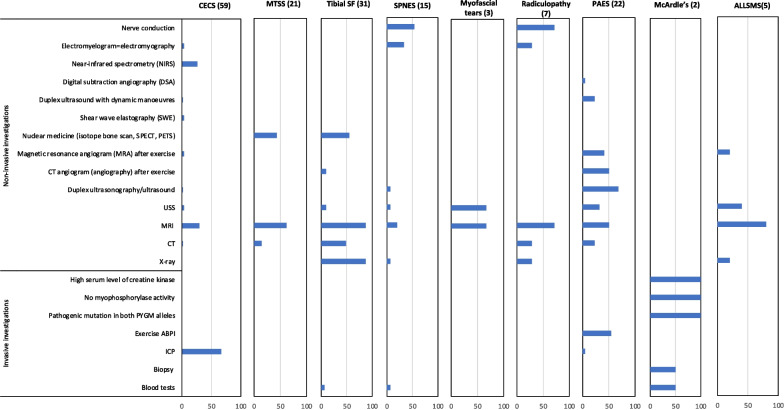
Methods: Three online databases were searched from inception to April 2022 for any English language original manuscripts identifying, describing, or assessing the clinical presentation and diagnostic criteria of the nine most common conditions that cause EILP. We included manuscripts considering all adults with any reported diagnostic criteria for EILP in any setting. Methodological quality was assessed using the Mixed Method Appraisal tool. Condition definitions were identified and categorised during data charting. Twenty-five potential elements of the history, 24 symptoms, 41 physical signs, 21 investigative tools, and 26 overarching diagnostic criteria, were identified and coded as counts of recommendation per condition, alongside qualitative analysis of the clinical reasoning. Condition definitions were constructed with 11 standardised elements based on recent consensus exercises for other conditions.
Results: One hundred nineteen retained manuscripts, of which 18 studied multiple conditions, had a median quality of 2/5. A combination of the history, pain location, symptoms, physical findings, and investigative modalities were fundamental to identify each sub-diagnosis alongside excluding differentials. The details differed markedly for each sub-diagnosis. Fifty-nine manuscripts included data on chronic exertional compartment syndrome (CECS) revealing exertional pain (83% history), dull aching pain (76% symptoms), absence of physical signs (78% physical findings) and elevated intercompartment pressure (93% investigative modality). Twenty-one manuscripts included data on medial tibial stress syndrome (MTSS), revealing persistent pain upon discontinuation of activity (81% history), diffuse medial tibial pain (100% pain location), dull ache (86% symptoms), diffuse tenderness (95% physical findings) and MRI for exclusion of differentials (62% investigative modality). Similar analyses were performed for stress fractures (SF, n = 31), popliteal artery entrapment syndrome (PAES, n = 22), superficial peroneal nerve entrapment syndrome (SPNES, n = 15), lumbar radiculopathy (n = 7), accessory/low-lying soleus muscle syndrome (ALLSMS, n = 5), myofascial tears (n = 3), and McArdle's syndrome (n = 2).
Conclusion: Initial diagnostic frameworks and definitions have been developed for each condition of the nine most common conditions that cause EILP, suitable for clinical consideration and consensus confirmation.
Keywords: Chronic exertional compartment syndrome; Exercise induced leg pain; Lumbar-sacral radiculopathy; McArdle’s syndrome; Medial tibial stress syndrome; Myofascial tears and accessory/low-lying soleus muscle syndrome; Popliteal artery entrapment syndrome; Superficial peroneal nerve entrapment syndrome; Tibial stress fractures.
© 2023. The Author(s).
Conflict of interest statement
Not applicable.
Figures



References
-
- Rajasekaran S, Kvinlaug K, Finnoff JT. Exertional leg pain in the athlete. PM R. 2012;4(12):985–1000. 10.1016/j.pmrj.2012.10.002. - PubMed
-
- Lohrer H, Malliaropoulos N, Korakakis V, Padhiar N. Exercise-induced leg pain in athletes: diagnostic, assessment, and management strategies. Phys Sportsmed. 2019;47(1):47–59. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
