

Effectiveness of Neural Mobilisation on Pain Intensity, Functional Status, and Physical Performance in Adults with Musculoskeletal Pain - A Systematic Review with Meta-Analysis
- PMID: 37990512
- PMCID: PMC10725147
- DOI: 10.1177/02692155231215216
Effectiveness of Neural Mobilisation on Pain Intensity, Functional Status, and Physical Performance in Adults with Musculoskeletal Pain - A Systematic Review with Meta-Analysis
Abstract
Objective: To investigate up-to-date evidence of the effectiveness of neural mobilisation techniques compared with any type of comparator in improving pain, function, and physical performance in people with musculoskeletal pain.
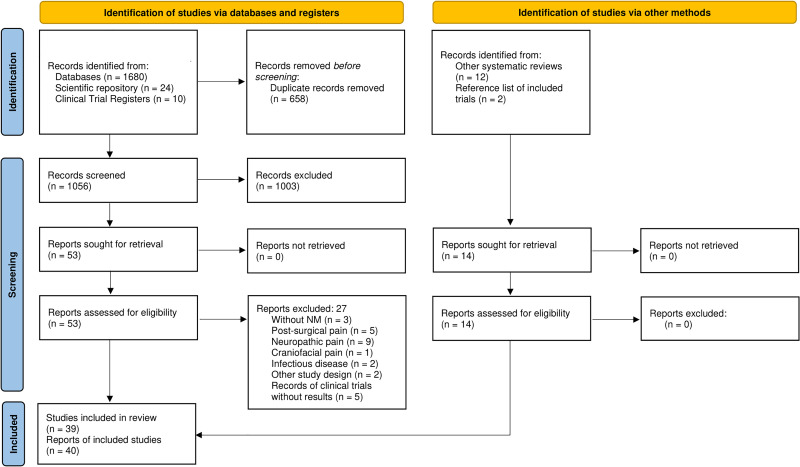
Data sources: The following sources were consulted: PubMed, Web of Science, CENTRAL, CINAHL, Scopus, and PEDro databases; scientific repositories; and clinical trial registers. The last search was performed on 01/06/2023.
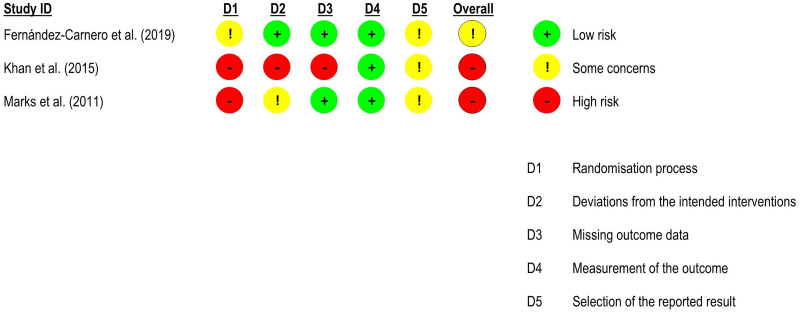
Methods: Two reviewers independently assessed the studies for inclusion. We included randomised, quasi-randomised, and crossover trials on musculoskeletal pain in which at least one group received neural mobilisation (alone or as part of multimodal interventions). Meta-analyses were performed where possible. The RoB 2 and the Grading of Recommendations Assessment, Development and Evaluation tools were used to assess risk of bias and to rate the certainty of evidence, respectively.
Results: Thirty-nine trials were identified. There was a significant effect favouring neural mobilisation for pain and function in people with low back pain, but not for flexibility. For neck pain, there was a significant effect favouring neural mobilisation as part of multimodal interventions for pain, but not for function and range of motion. Regarding other musculoskeletal conditions, it was not possible to conclude whether neural mobilisation is effective in improving pain and function. There was very low confidence for all effect estimates.
Conclusions: Neural mobilisation as part of multimodal interventions appears to have a positive effect on pain for patients with low back pain and neck pain and on function in people with low back pain. For the other musculoskeletal conditions, results are inconclusive.
Keywords: Physical therapy; disability; musculoskeletal disorders; neural mobilisation; pain.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures











Similar articles
-
Clinical effectiveness of manipulation and mobilisation interventions for the treatment of non-specific neck pain: protocol for a systematic review and meta-analysis.BMJ Open. 2020 Oct 10;10(10):e037783. doi: 10.1136/bmjopen-2020-037783. BMJ Open. 2020. PMID: 33040001 Free PMC article.
-
Effectiveness of neural mobilization on pain intensity, disability, and physical performance in adults with musculoskeletal pain-A protocol for a systematic review of randomized and quasi-randomized controlled trials and planned meta-analysis.PLoS One. 2022 Mar 10;17(3):e0264230. doi: 10.1371/journal.pone.0264230. eCollection 2022. PLoS One. 2022. PMID: 35271600 Free PMC article.
-
The effectiveness of neural mobilizations in the treatment of musculoskeletal conditions: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):65-75. doi: 10.11124/jbisrir-2015-1401. JBI Database System Rev Implement Rep. 2015. PMID: 26447008
-
Effects of kinesio taping alone versus sham taping in individuals with musculoskeletal conditions after intervention for at least one week: a systematic review and meta-analysis.Physiotherapy. 2019 Dec;105(4):412-420. doi: 10.1016/j.physio.2019.04.001. Epub 2019 Apr 8. Physiotherapy. 2019. PMID: 31076093
-
Workplace interventions for increasing standing or walking for decreasing musculoskeletal symptoms in sedentary workers.Cochrane Database Syst Rev. 2019 Nov 17;2019(11):CD012487. doi: 10.1002/14651858.CD012487.pub2. Cochrane Database Syst Rev. 2019. PMID: 31742666 Free PMC article.
Cited by
-
Demographic and Occupational Determinants of Work-Related Musculoskeletal Disorders: A Cross-Sectional Study.J Funct Morphol Kinesiol. 2025 Apr 20;10(2):137. doi: 10.3390/jfmk10020137. J Funct Morphol Kinesiol. 2025. PMID: 40566433 Free PMC article.
-
Effects of neural mobilization of sciatic nerve and its branches in plantar foot pressures and stabilometry.Sci Rep. 2024 Oct 8;14(1):23417. doi: 10.1038/s41598-024-72848-4. Sci Rep. 2024. PMID: 39379413 Free PMC article. Clinical Trial.
-
Perineural Electrical Dry Needling and Neural Mobilization for Chemotherapy-Induced Peripheral Neuropathy: Case Report.J Clin Med. 2025 Mar 28;14(7):2318. doi: 10.3390/jcm14072318. J Clin Med. 2025. PMID: 40217767 Free PMC article.
References
-
- World Health Organization. Musculoskeletal health, https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (2022).
-
- Hodges PW, Tucker K. Moving differently in pain: a new theory to explain the adaptation to pain. Pain 2011; 152: S90–S98. - PubMed
-
- Institute for Health Metrics And Evaluation. GBD 2019, https://vizhub.healthdata.org/gbd-compare/ (2019, accessed 2 August 2022).
-
- Institute for Health Metrics And Evaluation. WHO Rehabilitation Need Estimator, https://vizhub.healthdata.org/rehabilitation/ (2019, accessed 2 August 2022).
-
- de Kok J, Vroonhof P, Snijders J, et al. Work-related musculoskeletal disorders: prevalence, costs and demographics in the EU, 10.2802/66947 (2020). - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
