

A Trial-Based Cost-Utility Analysis of a Medication Optimization Intervention Versus Standard Care in Older Adults
- PMID: 37991657
- PMCID: PMC10682290
- DOI: 10.1007/s40266-023-01077-7
A Trial-Based Cost-Utility Analysis of a Medication Optimization Intervention Versus Standard Care in Older Adults
Abstract
Background: Older adults are at greater risk of medication-related harm than younger adults. The Integrated Medication Management model is an interdisciplinary method aiming to optimize medication therapy and improve patient outcomes.
Objective: We aimed to investigate the cost effectiveness of a medication optimization intervention compared to standard care in acutely hospitalized older adults.
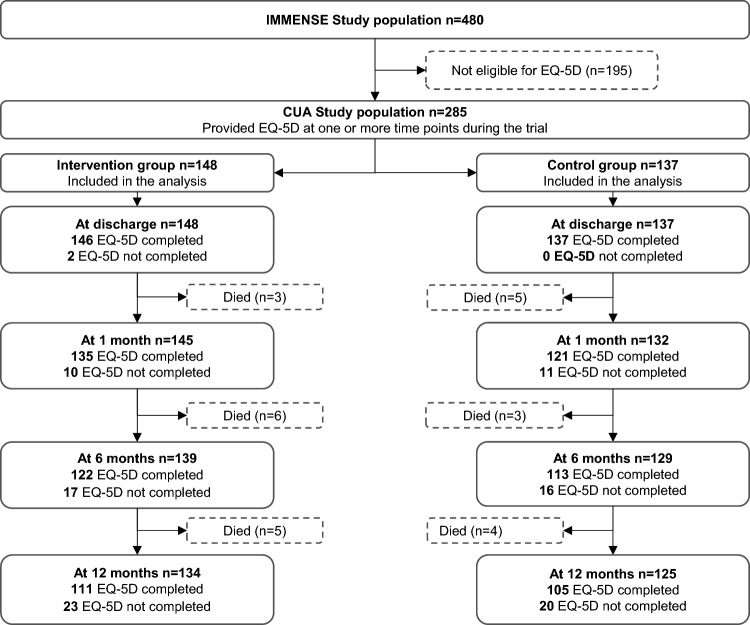
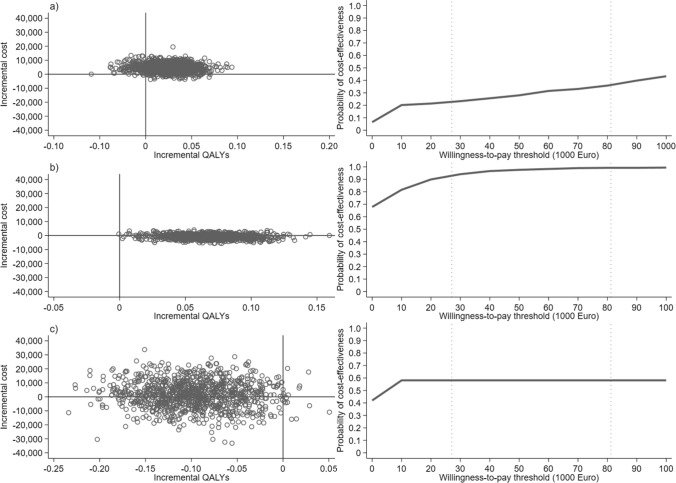
Methods: A cost-utility analysis including 285 adults aged ≥ 70 years was carried out alongside the IMMENSE study. Quality-adjusted life years (QALYs) were derived using the EuroQol 5-Dimension 3-Level Health State Questionnaire (EQ-5D-3L). Patient-level data for healthcare use and costs were obtained from administrative registers, taking a healthcare perspective. The incremental cost-effectiveness ratio was estimated for a 12-month follow-up and compared to a societal willingness-to-pay range of €/QALY 27,067-81,200 (NOK 275,000-825,000). Because of a capacity issue in a primary care resulting in extended hospital stays, a subgroup analysis was carried out for non-long and long stayers with hospitalizations < 14 days or ≥ 14 days.
Results: Mean QALYs were 0.023 [95% confidence interval [CI] 0.022-0.025] higher and mean healthcare costs were €4429 [95% CI - 1101 to 11,926] higher for the intervention group in a full population analysis. This produced an incremental cost-effectiveness ratio of €192,565/QALY. For the subgroup analysis, mean QALYs were 0.067 [95% CI 0.066-0.070, n = 222] and - 0.101 [95% CI - 0.035 to 0.048, n = 63] for the intervention group in the non-long stayers and long stayers, respectively. Corresponding mean costs were €- 824 [95% CI - 3869 to 2066] and €1992 [95% CI - 17,964 to 18,811], respectively. The intervention dominated standard care for the non-long stayers with a probability of cost effectiveness of 93.1-99.2% for the whole willingness-to-pay range and 67.8% at a zero willingness to pay. Hospitalizations were the main cost driver, and readmissions contributed the most to the cost difference between the groups.
Conclusions: According to societal willingness-to-pay thresholds, the medication optimization intervention was not cost effective compared to standard care for the full population. The intervention dominated standard care for the non-long stayers, with a high probability of cost effectiveness.
Clinical trial registration: The IMMENSE trial was registered in ClinicalTrials.gov on 28 June, 2016 before enrolment started (NCT02816086).
© 2023. The Author(s).
Conflict of interest statement
Eirin Guldsten Robinson, Hanna Gyllensten, Jeanette Schultz Johansen, Kjerstin Havnes, Anne Gerd Granas, Trine Strand Bergmo, Lars Småbrekke, Beate Hennie Garcia, and Kjell H. Halvorsen have no conflicts of interest that are directly relevant to the content of this article.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
