

A comprehensive model for assessing and classifying patients with thrombotic microangiopathy: the TMA-INSIGHT score
- PMID: 37993892
- PMCID: PMC10664252
- DOI: 10.1186/s12959-023-00564-6
A comprehensive model for assessing and classifying patients with thrombotic microangiopathy: the TMA-INSIGHT score
Abstract
Background: Thrombotic Microangiopathy (TMA) is a syndrome characterized by the presence of anemia, thrombocytopenia and organ damage and has multiple etiologies. The primary aim is to develop an algorithm to classify TMA (TMA-INSIGHT score).
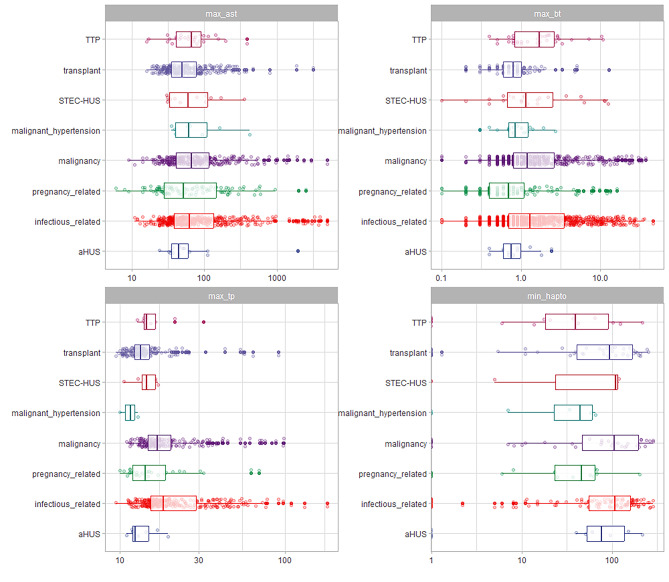
Methods: This was a single-center retrospective cohort study including hospitalized patients with TMA at a single center. We included all consecutive patients diagnosed with TMA between 2012 and 2021. TMA was defined based on the presence of anemia (hemoglobin level < 10 g/dL) and thrombocytopenia (platelet count < 150,000/µL), signs of hemolysis, and organ damage. We classified patients in eight categories: infections; Malignant Hypertension; Transplant; Malignancy; Pregnancy; Thrombotic Thrombocytopenic Purpura (TTP); Shiga toxin-mediated hemolytic uremic syndrome (STEC-SHU) and Complement Mediated TMA (aHUS). We fitted a model to classify patients using clinical characteristics, biochemical exams, and mean arterial pressure at presentation.
Results: We retrospectively retrieved TMA phenotypes using automatic strategies in electronic health records in almost 10 years (n = 2407). Secondary TMA was found in 97.5% of the patients. Primary TMA was found in 2.47% of the patients (TTP and aHUS). The best model was LightGBM with accuracy of 0.979, and multiclass ROC-AUC of 0.966. The predictions had higher accuracy in most TMA classes, although the confidence was lower in aHUS and STEC-HUS cases.
Conclusion: Secondary conditions were the most common etiologies of TMA. We retrieved comorbidities, associated conditions, and mean arterial pressure to fit a model to predict TMA and define TMA phenotypic characteristics. This is the first multiclass model to predict TMA including primary and secondary conditions.
Keywords: Atypical hemolytic uremic syndrome; Complement mediated TMA; Shiga toxin-mediated hemolytic uremic syndrome; Thrombotic Thrombocytopenic Purpura; Thrombotic microangiopathy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
LinkOut - more resources
Full Text Sources
