Guideline
doi: 10.5090/jcs.23.127.
Epub 2023 Nov 23.
2023 KASNet Guidelines on Atrial Fibrillation Surgery
Affiliations
- PMID: 37994091
- PMCID: PMC10792381
- DOI: 10.5090/jcs.23.127
Item in Clipboard
Guideline
2023 KASNet Guidelines on Atrial Fibrillation Surgery
J Chest Surg.
.
No abstract available
Keywords: Aortic valve disease; Atrial fibrillation; Congenital heart disease; Coronary disease; Cox-maze procedure; Degenerative mitral valve disease; Guidelines; Isolated atrial fibrillation surgery; Left atrial appendage; Rheumatic mitral valve disease; Surgical ablation; Ventricular tachycardia.
Conflict of interest statement
Jae Woong Choi, Ho Jin Kim, Joon Bum Kim, Han Ki Park is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
Figures
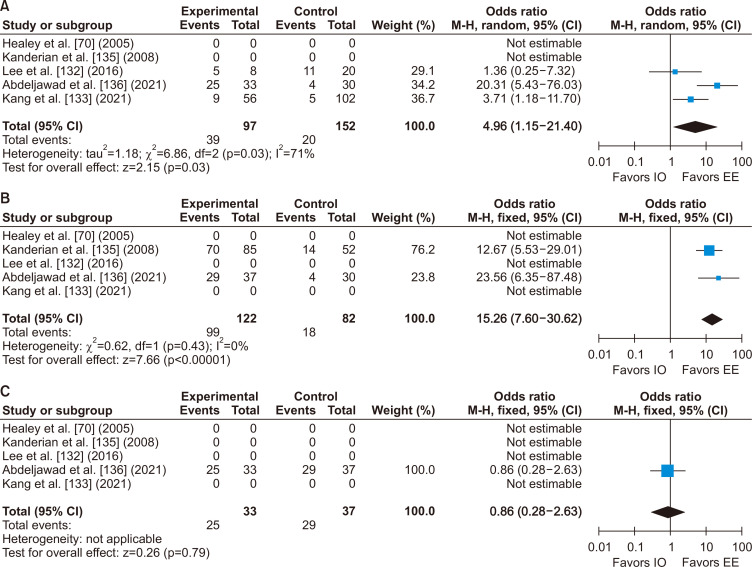
Forest plots for the risk of overall elimination failure rate of left atrial appendage (LAA) using (A) internal obliteration (IO) vs. external excision (EE), (B) external obliteration (EO) vs. external excision, and (C) IO vs. EO. The pooled estimates showed that the risk was significantly lower using EE than using the other techniques. M-H, Mantel-Haenszel; CI, confidence interval; df, degrees of freedom.
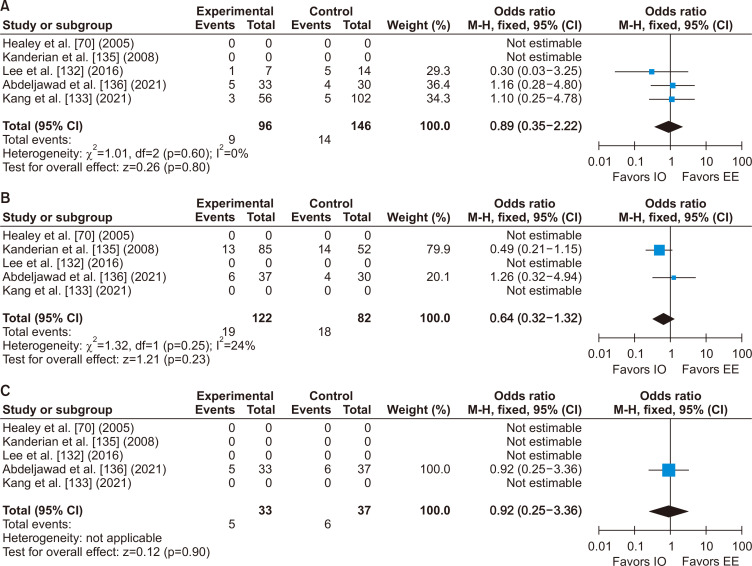
Forest plots for the risk of individual outcome of residual stumps after left atrial appendage (LAA) elimination using (A) internal obliteration (IO) vs. external excision (EE), (B) external obliteration (EO) vs. external excision, and (C) IO vs. EO. The pooled estimates showed that the risk did not show statistically significant differences among the 3 techniques. M-H, Mantel-Haenszel; CI, confidence interval; df, degrees of freedom.
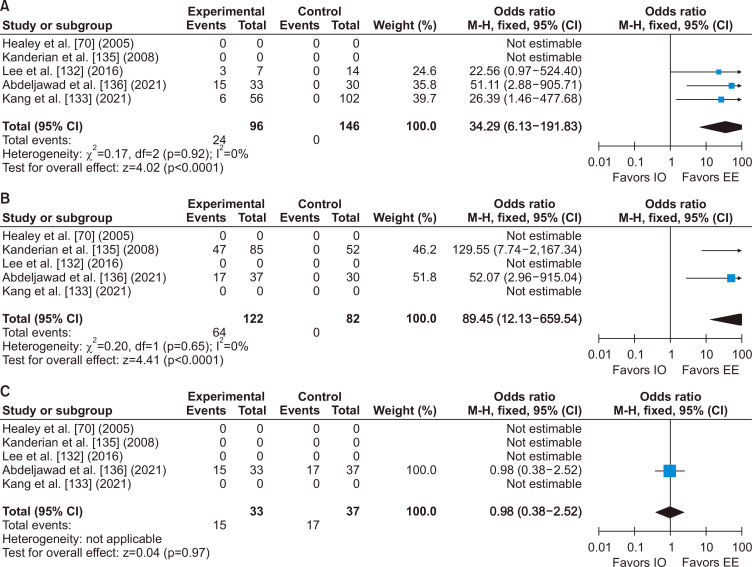
Forest plots for the risk of individual outcome of persistent gap or flow after left atrial appendage (LAA) elimination using (A) internal obliteration (IO) vs. external excision (EE), (B) external obliteration (EO) vs. external excision, and (C) IO vs. EO. The pooled estimates showed that the risk did not show statistically significant differences among the 3 techniques. M-H, Mantel-Haenszel; CI, confidence interval; df, degrees of freedom.
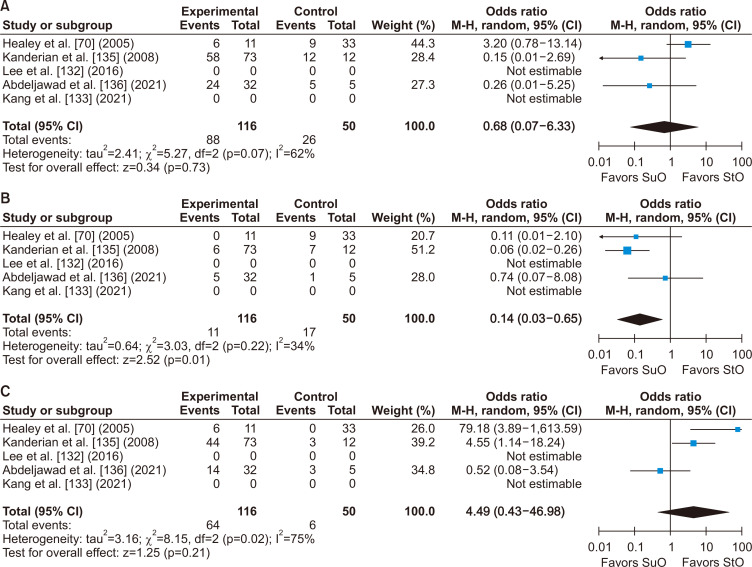
Forest plots for the risks of (A) overall elimination failure rate of left atrial appendage (LAA), (B) individual outcome of residual stump, and (C) individual outcome of persistent gap or flow after LAA elimination using external suture obliteration (SuO) vs. stapler obliteration (StO). The pooled estimates showed that the risk of residual stump was lower after SuO than after StO, while the other outcomes were not significantly different between the 2 techniques. M-H, Mantel-Haenszel; CI, confidence interval; df, degrees of freedom.
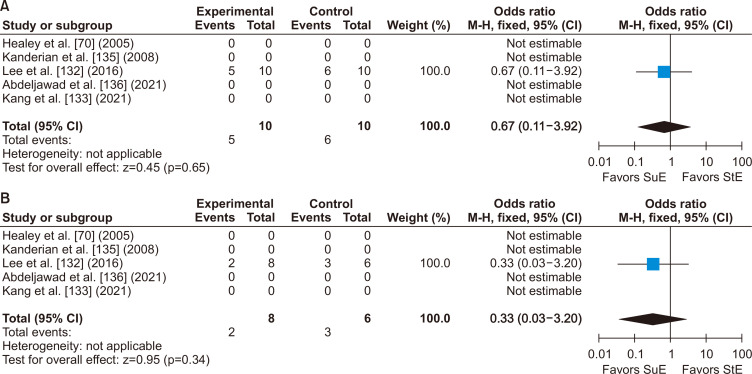
Forest plots for the risks of (A) overall elimination failure rate of left atrial appendage (LAA) and (B) individual outcome of residual stump after LAA elimination using external suture excision (SuE) vs. stapler excision (StE). The pooled estimates showed that the risks were not significantly different between the 2 techniques. M-H, Mantel-Haenszel; CI, confidence interval.
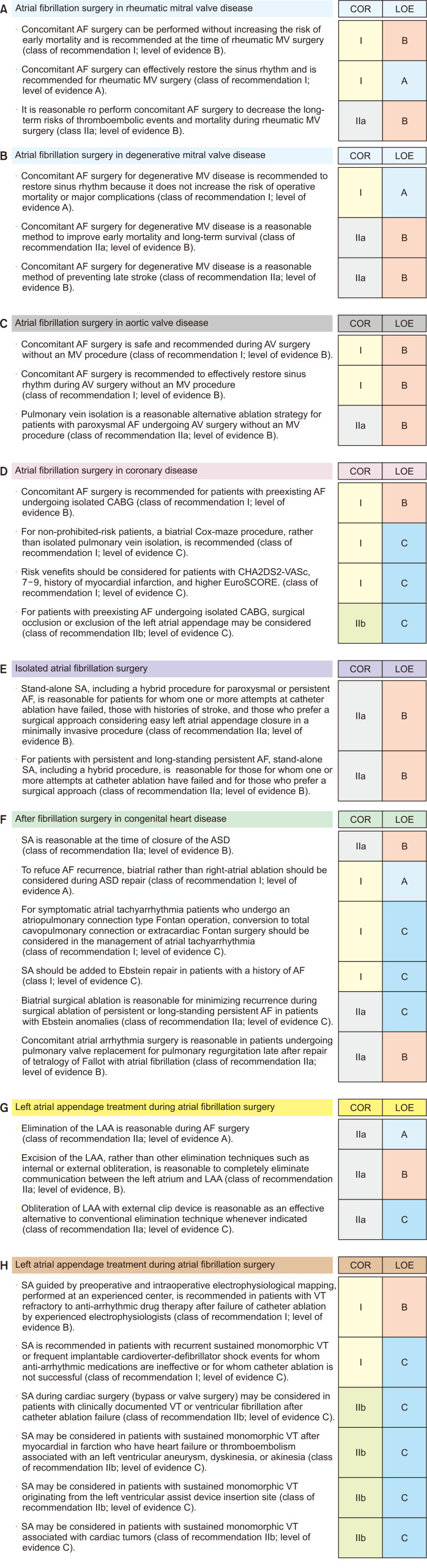
Recommendations regarding (A) atrial fibrillation (AF) surgery in rheumatic mitral valve (MV) disease, (B) AF surgery in degenerative MV disease, (C) AF surgery in aortic valve (AV) disease, (D) AF surgery in coronary disease, (E) isolated AF surgery, (F) AF surgery in congenital heart disease, (G) left atrial appendage (LAA) treatment during AF surgery, and (H) surgery for ventricular tachycardia (VT). CABG, coronary artery bypass grafting; SA, surgical ablation;ASD, atrial septal defect. (Continued on next page.)
References
-
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease, 1990-2015. N Engl J Med. 2017;377:713–22. doi: 10.1056/NEJMoa1603693. https://doi.org/10.1056/NEJMoa1603693. - DOI - PubMed
-
- Shenthar J. Management of atrial fibrillation in rheumatic heart disease. Heart Rhythm O2. 2022;3(6Part B):752–9. doi: 10.1016/j.hroo.2022.09.020. https://doi.org/10.1016/j.hroo.2022.09.020. - DOI - PMC - PubMed
-
- Oldgren J, Healey JS, Ezekowitz M, et al. Variations in cause and management of atrial fibrillation in a prospective registry of 15,400 emergency department patients in 46 countries: the RE-LY Atrial Fibrillation Registry. Circulation. 2014;129:1568–76. doi: 10.1161/CIRCULATIONAHA.113.005451. https://doi.org/10.1161/CIRCULATIONAHA.113.005451. - DOI - PubMed
-
- Badhwar V, Rankin JS, Damiano RJ, Jr, et al. The Society of Thoracic Surgeons 2017 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann Thorac Surg. 2017;103:329–41. doi: 10.1016/j.athoracsur.2016.10.076. https://doi.org/10.1016/j.athoracsur.2016.10.076. - DOI - PubMed
-
- Kim JY, Kim SH, Myong JP, et al. Ten-year trends in the incidence, treatment and outcomes of patients with mitral stenosis in Korea. Heart. 2020;106:746–50. doi: 10.1136/heartjnl-2019-315883. https://doi.org/10.1136/heartjnl-2019-315883. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources