

Life's essential 8 and risk of all-cause mortality in individuals with cardiovascular diseases: A prospective community-based study
- PMID: 37994466
- PMCID: PMC10823447
- DOI: 10.1002/clc.24119
Life's essential 8 and risk of all-cause mortality in individuals with cardiovascular diseases: A prospective community-based study
Abstract
Background: Although risk factors for mortality in individuals with cardiovascular diseases (CVD) have been reported, little is known regarding the association between the comprehensive cardiovascular health (CVH) index assessed by life's essential 8 (LE8) and the risk of mortality.
Hypothesis: The aim of this study was to evaluate the CVH assessed by LE8 and risk of mortality in individuals with CVD.
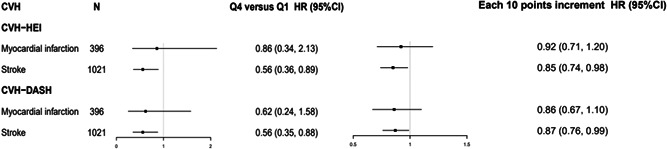
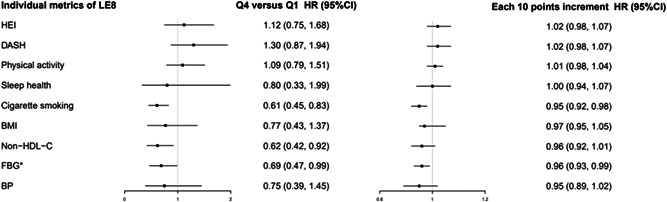
Methods: A total of 1391 participants with CVD diagnosed before 2014 from the Kailuan cohort were included in the analysis. The CVH score ranged from 0 to 100 was assessed using the LE8 metrics (diet quality, physical activity, sleep health, cigarette smoking, body mass index, lipids, blood glucose, and blood pressure). Cox regression model was used to estimate the association between the CVH score and risk of all-cause mortality.
Results: During a mean follow-up of 6.1 ± 1.5 years, 229 deaths occurred. The hazard ratio for all-cause mortality was 0.57 (95% confidence interval [CI]: 0.38, 0.84) in the highest quartiles compared with the lowest quartiles of CVH scores and 0.85 (95% CI: 0.75, 0.95) for each 10 points increment in CVH scores (ptrend = .009), after adjustment for age, sex, CVD duration, social-economic status, alcohol consumption, inflammation, medicine use, and kidney function. We did not observe significant interactions between the CVH scores and age, sex, and duration of CVD diagnosis (pinteraction > .05 for all).
Conclusions: The CVH assessed by the LE8 metrics was associated with a lower risk of all-cause mortality in individuals with CVD.
Keywords: all-cause mortality; cardiovascular disease; cardiovascular health; prevention.
© 2023 The Authors. Clinical Cardiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bonaccio M, Di Castelnuovo A, Costanzo S, et al. Interaction between Mediterranean diet and statins on mortality risk in patients with cardiovascular disease: findings from the Moli‐sani Study. Int J Cardiol. 2019;276:248‐254. - PubMed
-
- Bouabdallaoui N, Messas N, Greenlaw N, et al. Impact of smoking on cardiovascular outcomes in patients with stable coronary artery disease. Eur J Prev Cardiol. 2021;28(13):1460‐1466. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
