

Development and validation of a colorimetric antifungal susceptibility testing method for the dimorphic fungus Talaromyces marneffei
- PMID: 37994652
- PMCID: PMC10681740
- DOI: 10.1093/mmy/myad111
Development and validation of a colorimetric antifungal susceptibility testing method for the dimorphic fungus Talaromyces marneffei
Abstract
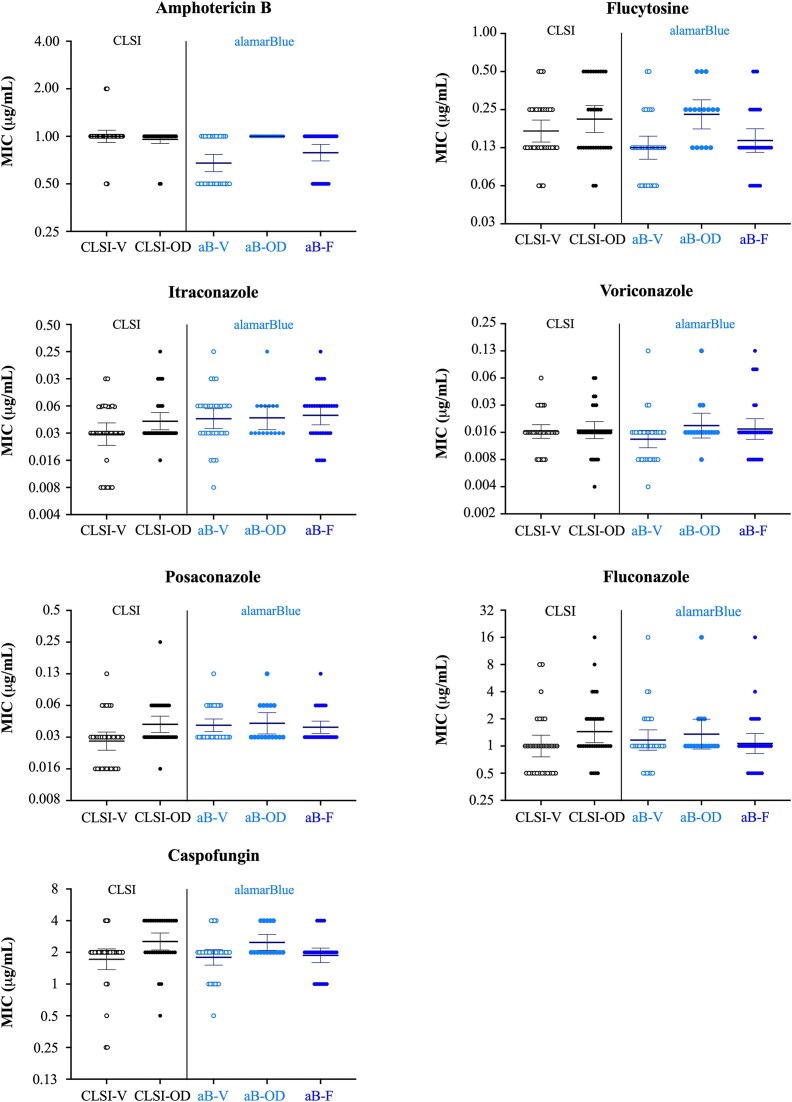
Antifungal drug resistance is an emerging cause of treatment failure in invasive fungal infections, and antifungal susceptibility testing (AFST) may inform treatment decisions. Currently, there are no established AFST guidelines for Talaromyces marneffei (Tm) or other dimorphic fungi. We developed a colorimetric AFST method using a fluorescent redox indicator alamarBlue, which changes from blue to pink in proportion to cellular metabolic activity. We determined the optimal time for alamarBlue addition to be 24 h post-inoculation and for MIC reading to be 72 h post-inoculation. Our method allows three ways to determine minimum inhibitory concentration (MIC): visual inspection of color change, optical density, and fluorescence intensity. We validated the assay by determining the MICs for seven antifungals against 32 Tm clinical isolates and assessed the essential agreement (EA) and inter-rater reliability between our alamarBlue and the Clinical Laboratory Standard Institute (CLSI) broth microdilution methods. The MIC ranges (from low to high) were: 0.008-0.025 μg/ml for itraconazole, 0.004-0.13 μg/ml for voriconazole, 0.03-0.13 μg/ml for posaconazole, 0.06-0.5 µg/ml for flucytosine, 0.5-1 µg/ml for amphotericin B, 0.5-4 µg/ml for caspofungin, and 0.5-16 µg/ml for fluconazole. The EAs were 100% between all three MIC readouts of the alamarBlue method, and 94%-100% between the alamarBlue and CLSI methods. Our alamarBlue method had substantially higher inter-rater agreement and offers a more reliable method that can be standardized across laboratories in both high- and low-resource settings compared to the established CLSI methodology.
Keywords: Talaromyces marneffei; Talaromycosis; antifungal susceptibility testing; dimorphic fungi.
Plain language summary
We developed a colorimetric alamarBlue method to determine the susceptibility of antifungal drugs against Talaromyces marneffei. We observed excellent agreement between the alamarBlue method and the Clinical Laboratory Standard Institute broth microdilution method, and the alamarBlue method had substantially higher inter-rater agreement.
© The Author(s) 2023. Published by Oxford University Press on behalf of The International Society for Human and Animal Mycology.
Figures



References
-
- Ning C, Wei W, Xu B, et al. The global distribution, drivers, and burden of talaromycosis 1964–2018. Presented at: Conference of Retrovirus and Opportunistic Infections, Boston, MA, US, March 8, 2020.
-
- Jiang J, Meng S, Huang S, et al. Effects of Talaromyces marneffei infection on mortality of HIV/AIDS patients in southern China: a retrospective cohort study. Clin Microbiol Infect. 2019; 25: 233–241. - PubMed
