

Surgery versus radiotherapy for limited-stage small cell esophageal carcinoma: a multicenter, retrospective, cohort study in China (ChiSCEC)
- PMID: 37995095
- PMCID: PMC10871645
- DOI: 10.1097/JS9.0000000000000912
Surgery versus radiotherapy for limited-stage small cell esophageal carcinoma: a multicenter, retrospective, cohort study in China (ChiSCEC)
Abstract
Background: There is no standard management for small cell esophageal carcinoma (SCEC). The purpose of this multicenter, retrospective study (ChiSCER) was to investigate the treatment, outcomes, and risk factors impacting survival endpoints in patients with limited-stage SCEC (LS-SCEC).
Materials and methods: Consecutive patients with LS-SCEC from 14 institutions between 2000 and 2020 in China were enrolled. Survival curves were constructed using the Kaplan-Meier method and compared using a log-rank test. Univariate and multivariate Cox regression models and propensity score matching (PSM) analysis were adopted in the prognostic analysis. Results were reported as hazard ratio (HR), 95% confidence interval (CI), and P value. Statistical significance was set as P value <0.05 in a two-tailed test.
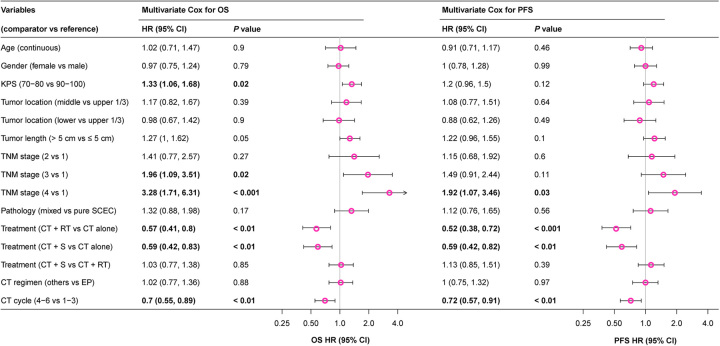
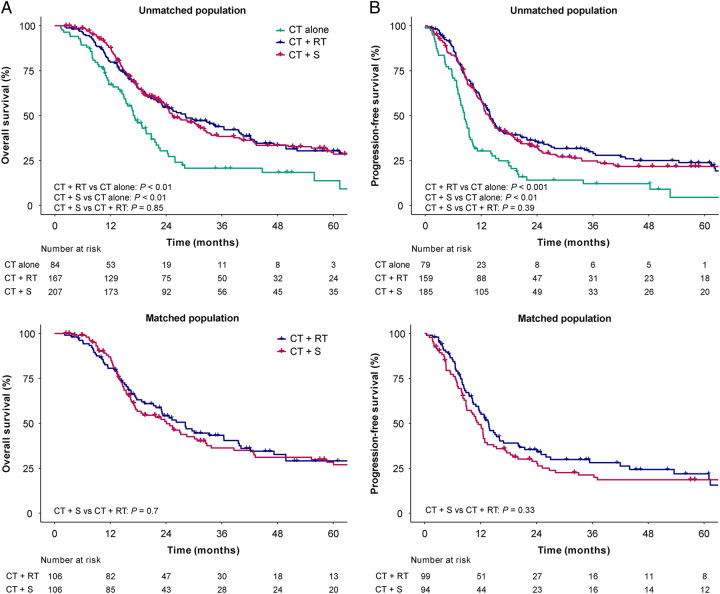
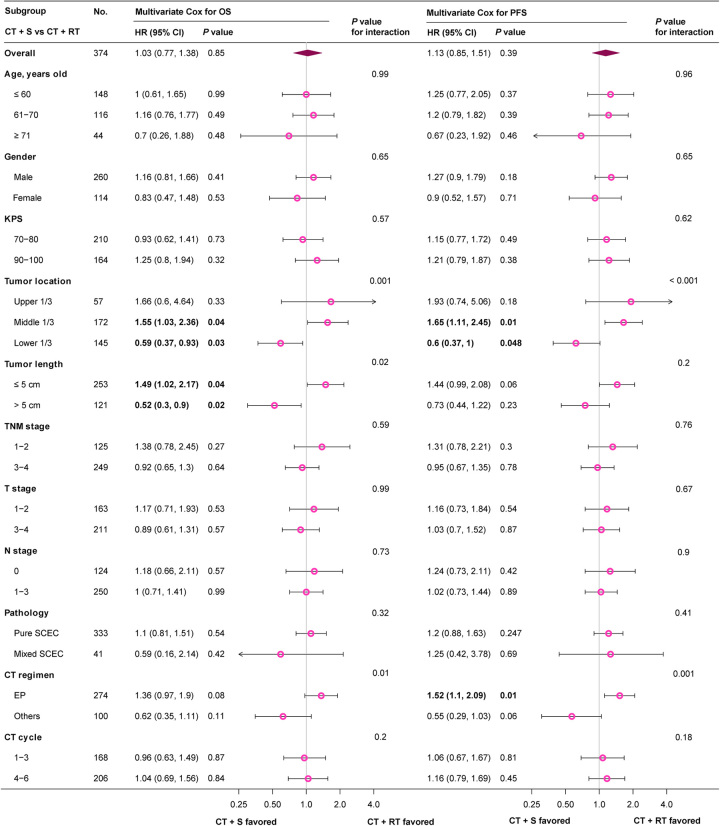
Results: Among 458 LS-SCEC patients, the median age was 63 [interquartile range (IQR), 57-68] years, and 318 (69%) were males. Eighty-four (18%), 167 (36%), and 207 (45%) patients received chemotherapy (CT) alone, CT plus definitive radiotherapy (CT+RT), and CT plus radical surgery (CT+S), respectively. With a median follow-up time of 58.7 (95% CI 48.9-68.6) months, the median overall survival (OS) and 3-year OS rate for all patients 24.3 (95% CI 21.6-27) months and 37.3% (95% CI 32.8-42.5%), respectively. Multivariate analysis indicated that treatment modes, Karnofsky performance status (KPS), TNM stage, and CT cycle were independent prognostic factors for OS ( P <0.05). Compared with CT alone, patients treated with CT+RT (HR 0.57, 95% CI 0.41-0.8, P =0.001) or CT+S (HR 0.59, 95% CI 0.42-0.82, P =0.002) had an improved OS, with no significant survival differences between CT+S and CT+RT groups after multivariate and PSM analyses ( P >0.05). Subgroup analysis indicated that compared with CT+RT, patients with tumor location at lower 1/3 (HR 0.59, 95% CI 0.37-0.93, P =0.03) or tumor length >5 cm (HR 0.52, 95% CI 0.3-0.9, P =0.02) could obtain significant OS benefit from CT+S. Patients with tumor location at middle 1/3 (HR 1.55, 95% CI 1.03-2.36, P =0.04) or tumor length ≤5 cm (HR 1.49, 95% CI 1.02-2.17, P =0.04) favored CT+RT. Distant metastasis accounted for 73.7% of all treatment failures after multidisciplinary treatments.
Conclusion: Surgery and RT were equally effective local therapies for patients with LS-SCEC. The personalized decision of local therapy should be made after comprehensive considerations on tumor location, length, comorbidities, and organ preservation.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Brenner B, Tang LH, Klimstra DS, et al. Small-cell carcinomas of the gastrointestinal tract: a review. J Clin Oncol 2004;22:2730–2739. - PubMed
-
- Kukar M, Groman A, Malhotra U, et al. Small cell carcinoma of the esophagus: a SEER database analysis. Ann Surg Oncol 2013;20:4239–4244. - PubMed
-
- Lv J, Liang J, Wang J, et al. Primary small cell carcinoma of the esophagus. J Thorac Oncol 2008;3:1460–1465. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
