

High serum C-X-C motif chemokine ligand 10 (CXCL10) levels may be associated with new onset interstitial lung disease in patients with systemic sclerosis: evidence from observational, clinical, transcriptomic and in vitro studies
- PMID: 37995465
- PMCID: PMC10708993
- DOI: 10.1016/j.ebiom.2023.104883
High serum C-X-C motif chemokine ligand 10 (CXCL10) levels may be associated with new onset interstitial lung disease in patients with systemic sclerosis: evidence from observational, clinical, transcriptomic and in vitro studies
Abstract
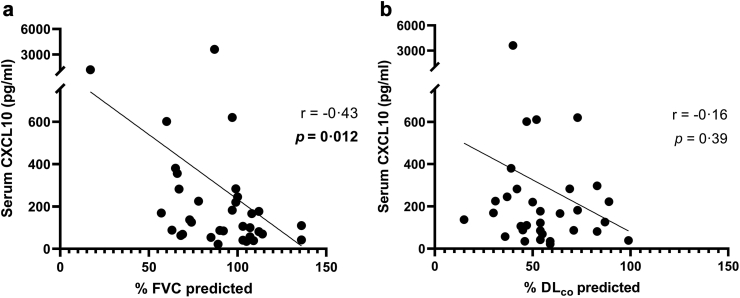
Background: Systemic sclerosis-interstitial lung disease (SSc-ILD) is the leading cause of death in patients with SSc. There is an unmet need for predictive biomarkers to identify patients with SSc at risk of ILD. Previous studies have shown that interferon (IFN) pathways may play a role in SSc. We assessed the use of C-X-C motif chemokine ligand 10 (CXCL10) as a predictive biomarker for new onset of ILD in patients with SSc.
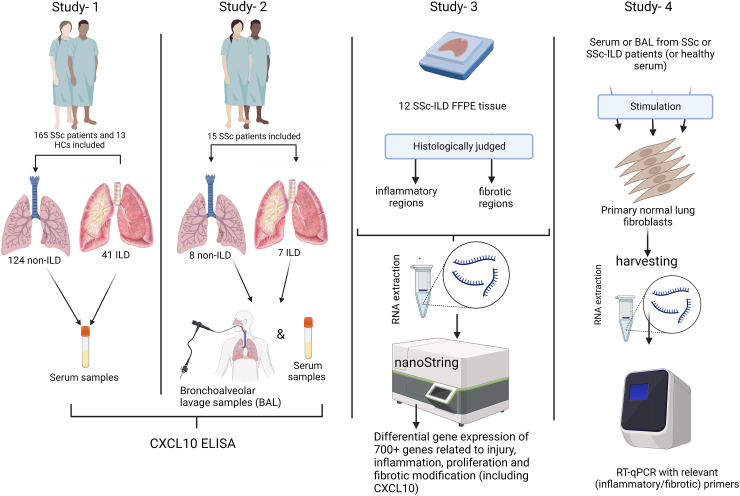
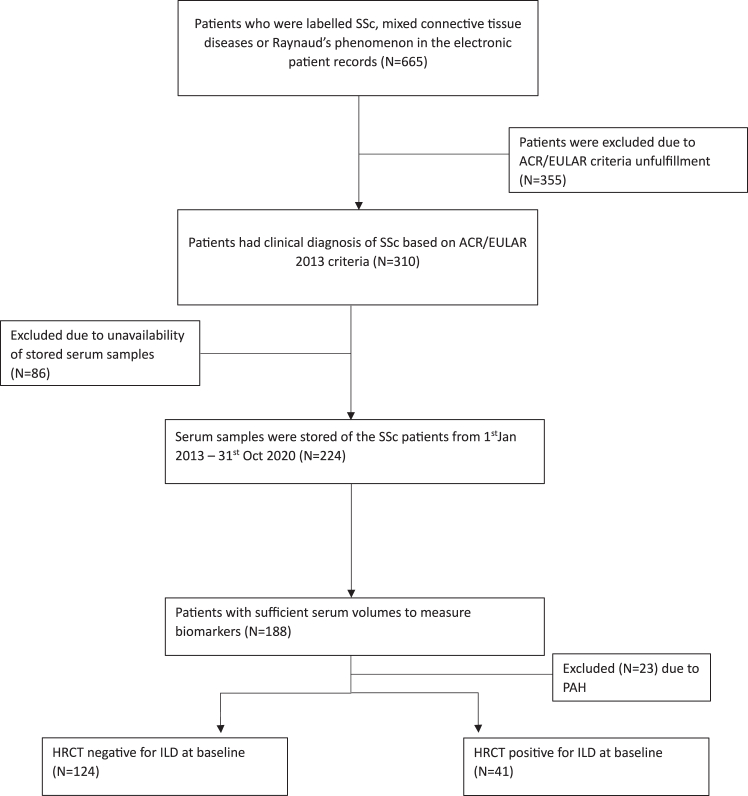
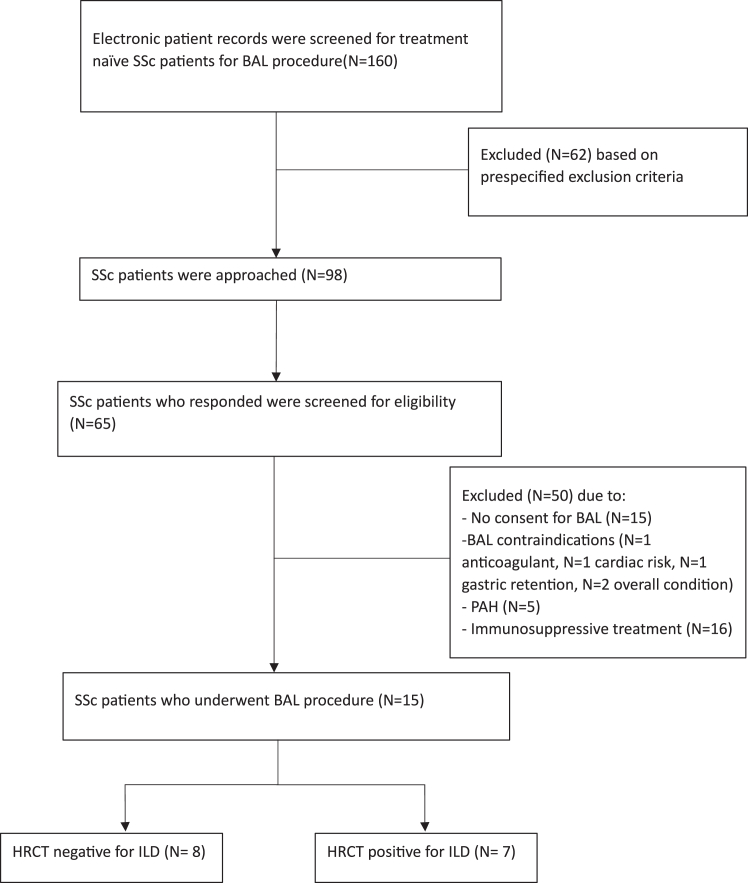
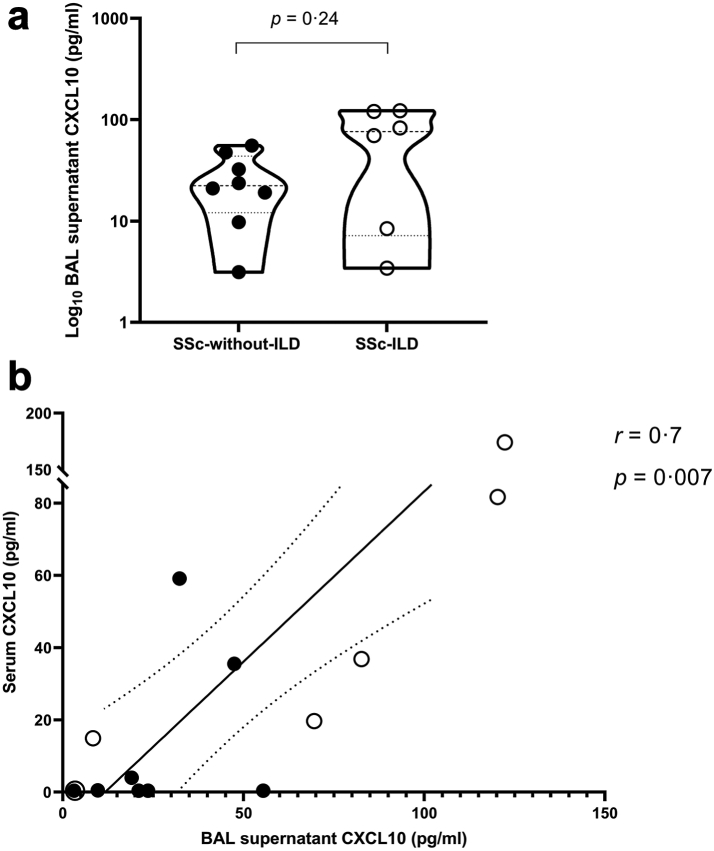
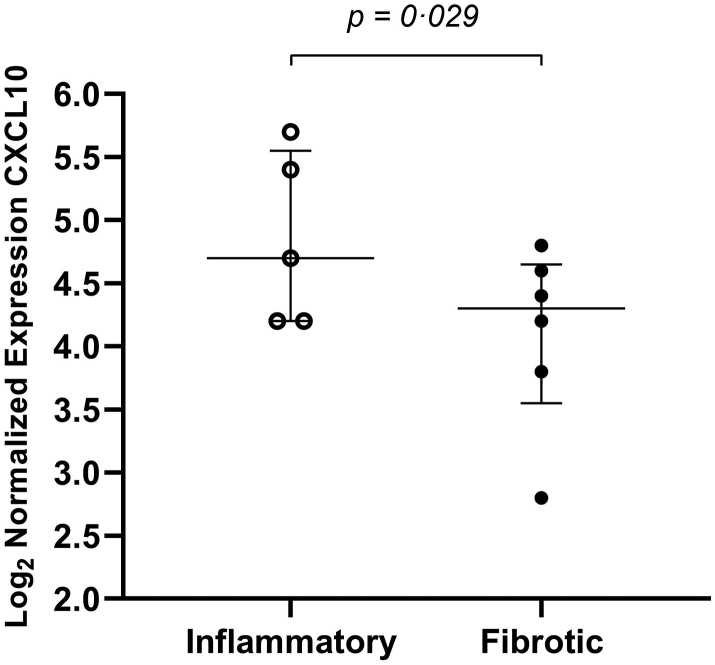
Methods: One-hundred-sixty-five (Female, N = 130) patients with SSc (SSc-ILD, N = 41) and 13 (Female, N = 8) healthy controls were investigated retrospectively. CXCL10 protein levels were measured by ELISA. We performed log rank analysis with baseline CXCL10 serum levels. CXCL10 nanoString data from lung tissues obtained from transplanted patients with SSc-ILD were extracted. Fifteen (Female, N = 10) patients with SSc (SSc-ILD, N = 7) were recruited for bronchoalveolar lavage (BAL) procedure. Lung fibroblasts were treated with BAL-fluid or serum from patients with SSc with or without ILD. Inflammatory/fibrotic genes were assessed.
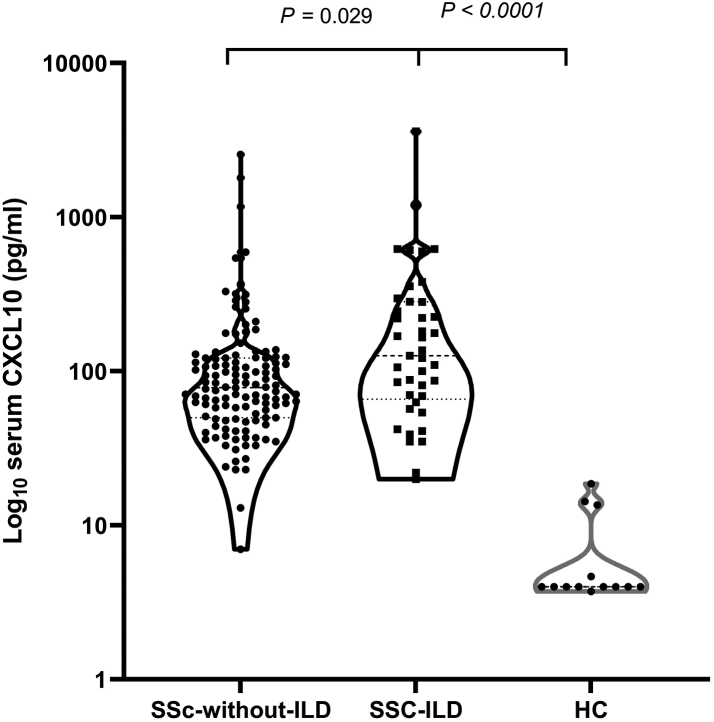
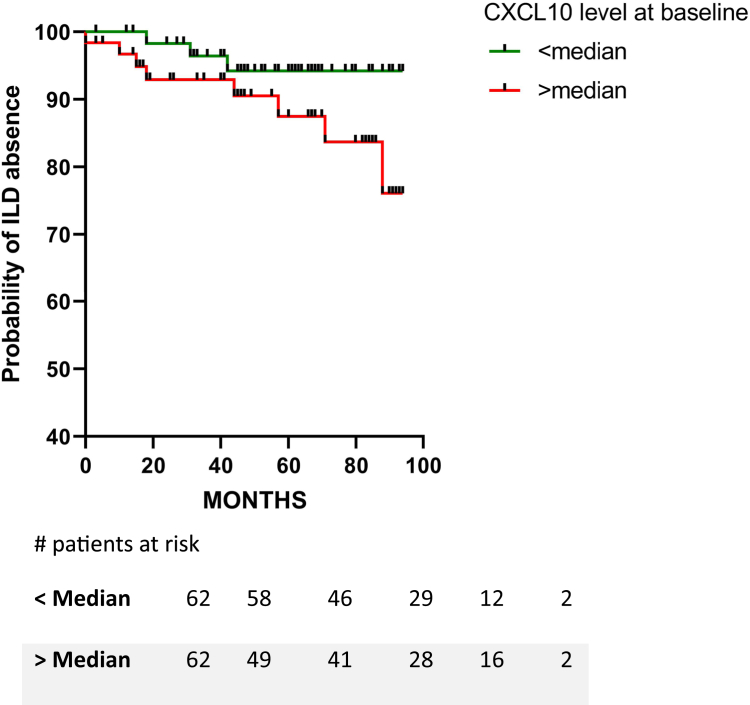
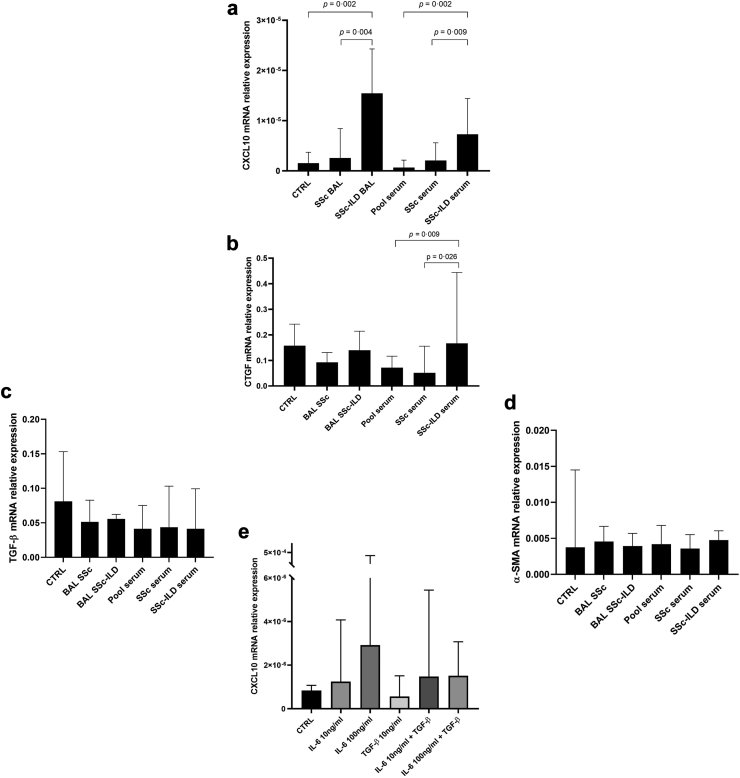
Findings: Serum CXCL10 levels were higher in patients with SSc-ILD compared to SSc patients without ILD [Median (IQR):126 pg/ml (66-282.5) vs. 78.5 pg/ml (50-122), P = 0.029, 95% CI: 1.5 × 10-6 to 0.4284]. Survival analysis showed that baseline CXCL10 levels >78.5 pg/ml have a 2.74-fold increased risk of developing new onset of ILD (Log-rank: P = 0.119) on follow-up. CXCL10 levels in BAL supernatant were not different in patients with SSc-ILD compared to SSc without ILD [76.1 pg/ml (7.2-120.8) vs. 22.3 pg/ml (12.1-43.7), P = 0.24, 95% CI: -19.5 to 100]. NanoString showed that CXCL10 mRNA expression was higher in inflammatory compared to fibrotic lung tissues [4.7 (4.2-5.6) vs. 4.3 (3.6-4.7), P = 0.029]. Fibroblasts treated with SSc-ILD serum or BAL fluids overexpressed CXCL10.
Interpretations: Clinical, transcriptomic, and in vitro data showed that CXCL10 is potentially involved in early SSc-ILD. More research is needed to confirm whether CXCL10 can be classified as a prospective biomarker to detect patients with SSc at higher risk of developing new onset ILD.
Funding: This collaborative project is co-financed by the Ministry of Economic Affairs and Climate Policy of the Netherlands utilizing the PPP-allowance made available by the Top Sector Life Sciences & Health to stimulate public-private partnerships (PPP-2019_007). Part of this study is financially supported by Sanofi Genzyme (NL8921).
Keywords: Biomarker; CXCL10; Fibrosis; ILD; Inflammation; Systemic sclerosis.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests D.J. Mulder received grants from Sanofi Genzyme paid to the institution. W. Timens received consultancy fees from Merck Sharp Dohme and Bristol-Myers Squibb. The rest of the coauthors declare no conflict of interest.
Figures
References
-
- Salazar G.A., Kuwana M., Wu M., et al. KL-6 but not CCL-18 is a predictor of early progression in systemic sclerosis-related interstitial lung disease. J Rheumatol. 2018;45(8):1153. http://www.jrheum.org/content/45/8/1153.abstract Available from: - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
