

Cellular mechanisms associated with sub-optimal immune responses to SARS-CoV-2 bivalent booster vaccination in patients with Multiple Myeloma
- PMID: 37995467
- PMCID: PMC10708991
- DOI: 10.1016/j.ebiom.2023.104886
Cellular mechanisms associated with sub-optimal immune responses to SARS-CoV-2 bivalent booster vaccination in patients with Multiple Myeloma
Abstract
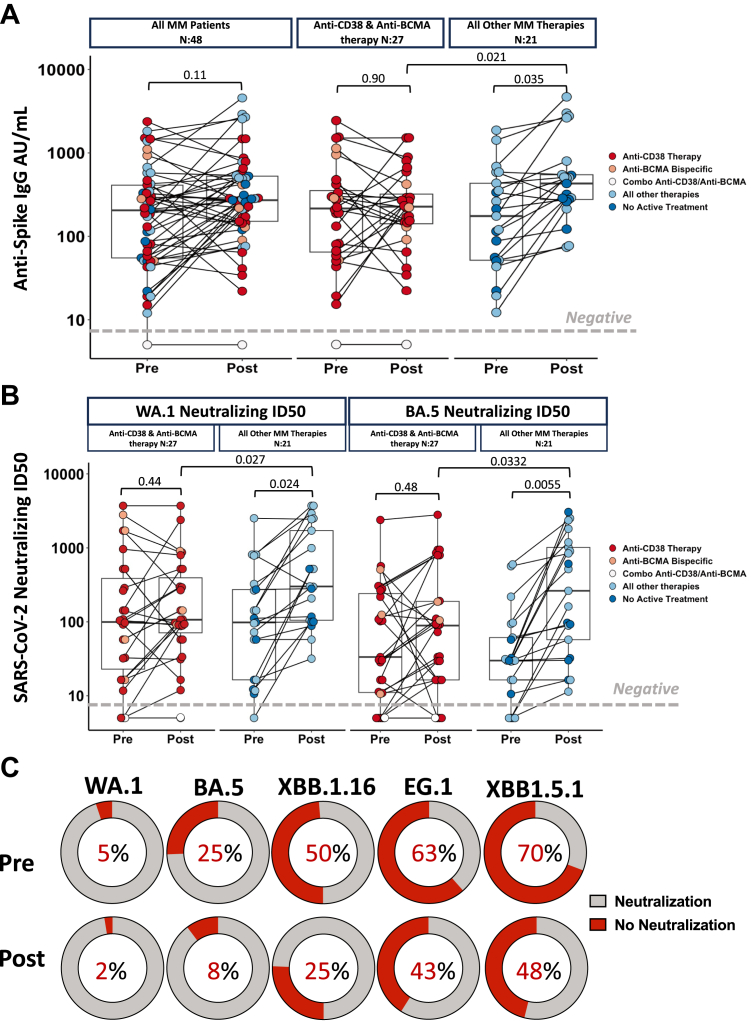
Background: The real-world impact of bivalent vaccines for wild type (WA.1) and Omicron variant (BA.5) is largely unknown in immunocompromised patients with Multiple Myeloma (MM). We characterize the humoral and cellular immune responses in patients with MM before and after receiving the bivalent booster, including neutralizing assays to identify patterns associated with continuing vulnerability to current variants (XBB1.16, EG5) in the current post-pandemic era.
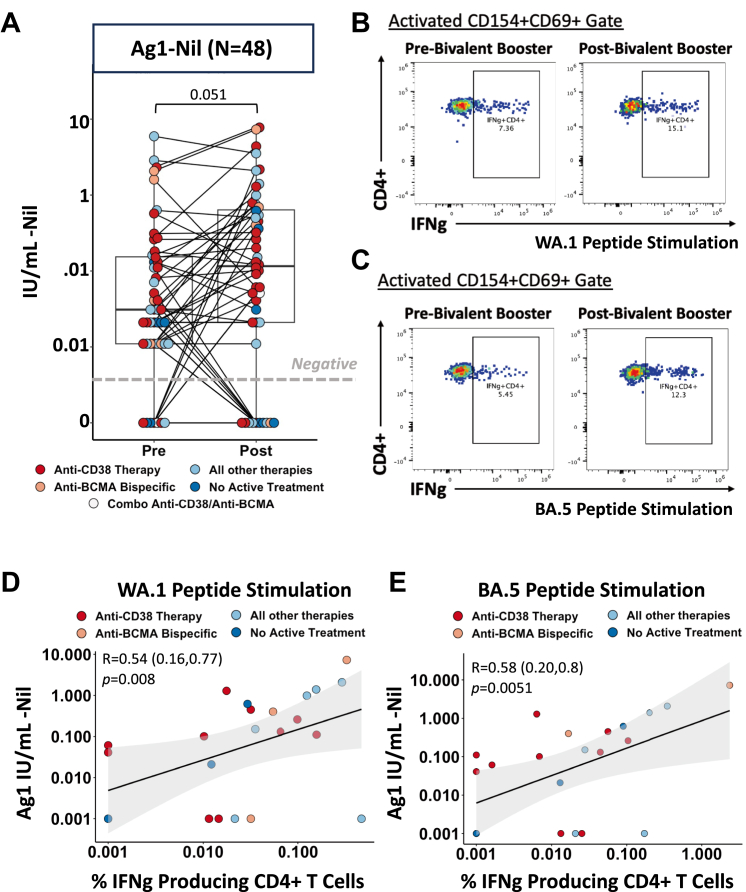
Methods: We studied the humoral and cellular immune responses before and after bivalent booster immunization in 48 MM patients. Spike binding IgG antibody levels were measured by SARS-CoV-2 spike binding ELISA and neutralization capacity was assessed by a SARS-CoV-2 multi-cycle microneutralization assays to assess inhibition of live virus. We measured spike specific T-cell function using the QuantiFERON SARS-CoV-2 (Qiagen) assay as well as flow-cytometry based T-cell. In a subset of 38 patients, high-dimensional flow cytometry was performed to identify immune cell subsets associated with lack of humoral antibodies.
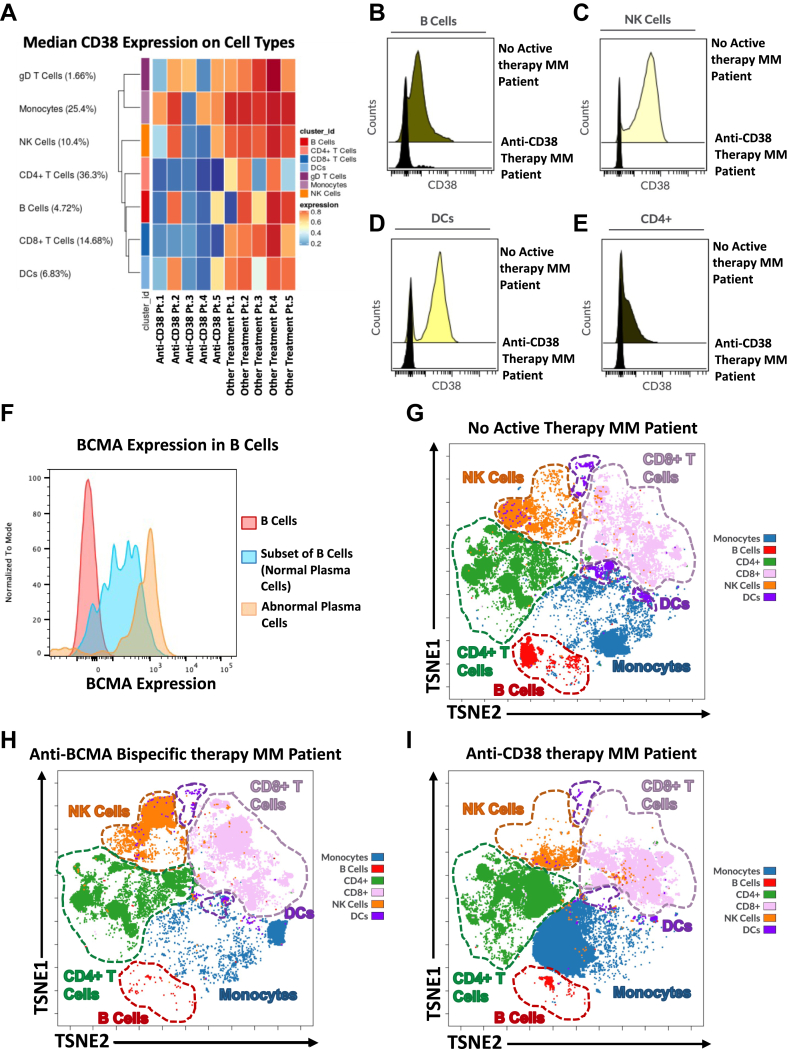
Findings: We find that bivalent vaccination provides significant boost in protection to the omicron variant in our MM patients, in a treatment specific manner. MM patients remain vulnerable to newer variants with mutations in the spike portion. Anti-CD38 and anti-BCMA therapies affect the immune machinery needed to produce antibodies.
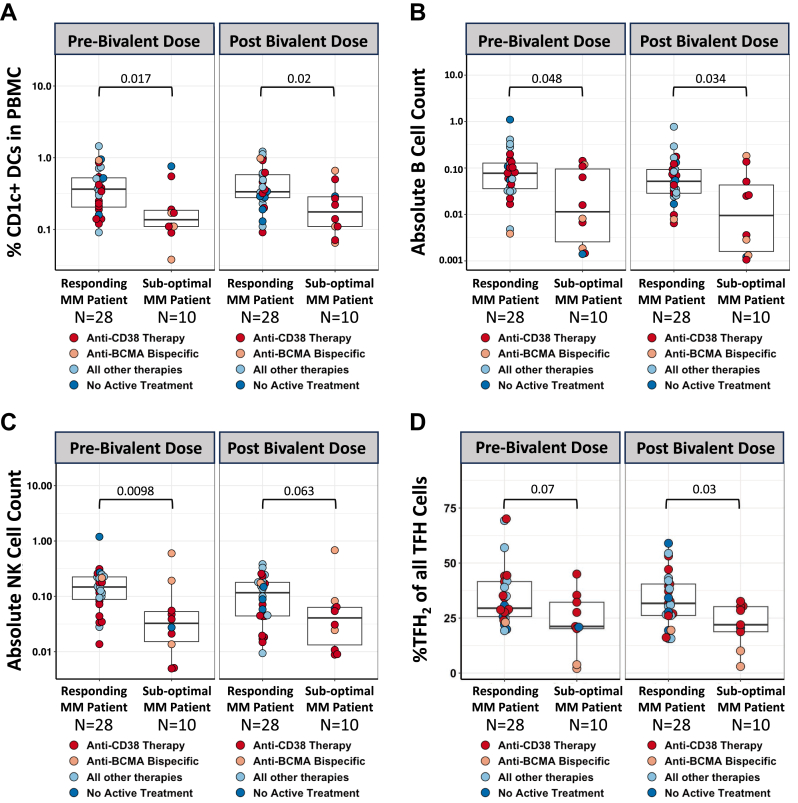
Interpretation: Our study highlights varying immune responses observed in MM patients after receiving bivalent COVID-19 vaccination. Specifically, a subgroup of MM patients undergoing anti-CD38 and anti-BCMA therapy experience impairment in immune cells such DCs, B cells, NK cells and TFH cells, leading to an inability to generate adequate humoral and cellular responses to vaccination.
Funding: National Cancer Institute (National Institutes of Health), National Institute of Allergy and Infectious Diseases (National Institutes of Health), NCI Serological Sciences Network for COVID-19 (SeroNet) and The Icahn School of Medicine at Mount Sinai.
Keywords: Bivalent vaccine; COVID-19; Hematological malignancy; Multiple Myeloma; Omicron; SARS-CoV-2.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests The Icahn School of Medicine at Mount Sinai has filed patent applications relating to SARS-CoV-2 serological assays which list Viviana Simon and Carlos Cardon-Cordo as co-inventors. Mount Sinai has spun out a company, Kantaro, to market serological tests for SARS-CoV-2. Sundar Jagannath reports consulting fees for Bristol Myers Squibb (Celgene), Janssen, Karyopharm Therapeutics, Merck, Sanofi, and Takeda Pharmaceuticals. Samir Parekh reports consulting fees from Foundation Medicine and research funding from Bristol Myers Squibb (Celgene), Karyopharm, and Amgen. The other authors reported no relevant conflicts of interest.
Figures
References
-
- Giuliani N., Accardi F., Marchica V., et al. Novel targets for the treatment of relapsing multiple myeloma. Expert Rev Hematol. 2019;12(7):481–496. - PubMed
-
- Shah U.A., Mailankody S. Emerging immunotherapies in multiple myeloma. BMJ. 2020;370 - PubMed
-
- Nucci M., Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009;49(8):1211–1225. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
