

Efficacy and safety of second-line cabozantinib after immuno-oncology combination therapy for advanced renal cell carcinoma: Japanese multicenter retrospective study
- PMID: 37996622
- PMCID: PMC10667220
- DOI: 10.1038/s41598-023-48087-4
Efficacy and safety of second-line cabozantinib after immuno-oncology combination therapy for advanced renal cell carcinoma: Japanese multicenter retrospective study
Abstract
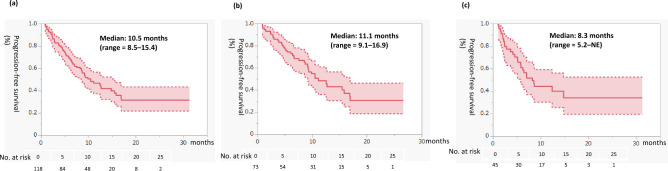
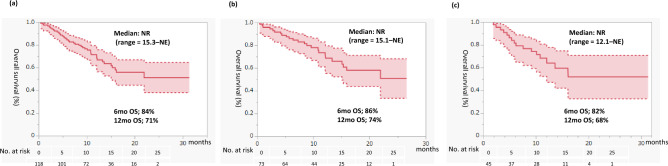
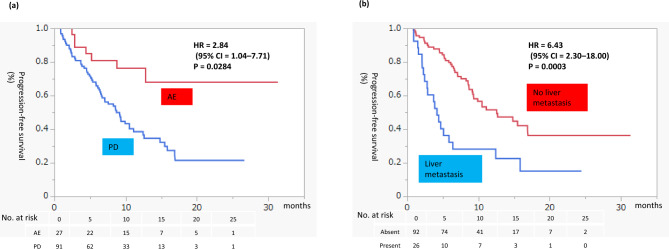
Immuno-oncology (IO) combination therapy is utilized as a first-line systemic treatment for advanced renal cell carcinoma. However, evidence supporting the use of cabozantinib after IO combination therapy is lacking. We retrospectively analyzed patients who received second-line cabozantinib after IO combination therapy using the Japanese Urological Oncology Group (JUOG) database. In total, 254 patients were enrolled in the JUOG global study, and 118 patients who received second-line cabozantinib comprised the study cohort. The objective response rate, disease control rate, second-line cabozantinib progression-free survival (PFS), and overall survival from second-line for overall were 32%, 75%, 10.5 months, and not reached, respectively, for first-line IO-IO therapy were 37%, 77%, 11.1 months, and not reached, respectively, versus 24%, 71%, 8.3 months, and not reached, respectively, for first-line IO-tyrosine kinase inhibitor therapy. In univariate and multivariate analyses, discontinuation of first-line treatment because of progressive disease and liver metastasis were independent risk factors for PFS. All-grade adverse events occurred in 72% of patients, and grade 3 or higher adverse events occurred in 28% of patients. Second line-cabozantinib after first-line IO combination therapy for advanced renal cell carcinoma was expected to be effective after either IO-IO or IO-TKI treatment and feasible in real-world practice.
© 2023. The Author(s).
Conflict of interest statement
Tomokazu Sazuka has received honoraria from Takeda and BMS. Takahiro Osawa has received honoraria from Takeda and ONO. Takahiro Kimura is a paid consultant/advisor of Astellas, AstraZeneca, Bayer, Janssen, and Sanofi. Masayuki Takahashi has received honoraria from MSD, Eizai, Merck and Pfizer. Kazutoshi Fujita has received honoraria from ONO, BMS, MSD, Pfizer and Takeda. Hiroshi Kitamura has received honoraria from BMS and MSD, Research expenses from BMS and MSD. The funders had no role in the design of the study; data collection, analysis, and interpretation; manuscript writing; or the decision to publish the results.
Figures
Similar articles
-
Combination antiangiogenic tyrosine kinase inhibition and anti-PD1 immunotherapy in metastatic renal cell carcinoma: A retrospective analysis of safety, tolerance, and clinical outcomes.Cancer Med. 2021 Apr;10(7):2341-2349. doi: 10.1002/cam4.3812. Epub 2021 Mar 1. Cancer Med. 2021. PMID: 33650321 Free PMC article.
-
Efficacy and Safety of Immuno-Oncology Plus Tyrosine Kinase Inhibitors as Late-Line Combination Therapy for Patients with Advanced Renal Cell Carcinoma.J Clin Med. 2024 Jun 7;13(12):3365. doi: 10.3390/jcm13123365. J Clin Med. 2024. PMID: 38929893 Free PMC article.
-
Changes in outcome of patients with advanced non-clear cell renal cell carcinoma from the tyrosine kinase inhibitor era to the immuno-oncology era.Int J Clin Oncol. 2024 Nov;29(11):1730-1739. doi: 10.1007/s10147-024-02606-z. Epub 2024 Aug 14. Int J Clin Oncol. 2024. PMID: 39143429
-
Median time to progression with TKI-based therapy after failure of immuno-oncology therapy in metastatic kidney cancer: A systematic review and meta-analysis.Eur J Cancer. 2021 Sep;155:245-255. doi: 10.1016/j.ejca.2021.07.014. Epub 2021 Aug 12. Eur J Cancer. 2021. PMID: 34392067
-
Cabozantinib plus Nivolumab: A Review in Advanced Renal Cell Carcinoma.Target Oncol. 2022 Mar;17(2):193-201. doi: 10.1007/s11523-022-00866-1. Epub 2022 Feb 17. Target Oncol. 2022. PMID: 35175500 Review.
Cited by
-
Second-Line Systemic Therapies in Metastatic Renal Cell Carcinoma: Current Insights and Future Directions.J Cancer Immunol (Wilmington). 2025;7(2):81-94. doi: 10.33696/cancerimmunol.7.107. J Cancer Immunol (Wilmington). 2025. PMID: 40661855 Free PMC article.
-
Real-world experience of second-line axitinib in metastatic renal cell carcinoma: analysis of the Swedish population.Future Oncol. 2024;20(20):1385-1392. doi: 10.1080/14796694.2024.2351352. Epub 2024 Jul 26. Future Oncol. 2024. PMID: 39057291 Free PMC article.
References
-
- Haanen J, et al. Extended follow-up from JAVELIN Renal 101: Subgroup analysis of avelumab plus axitinib versus sunitinib by the International Metastatic Renal Cell Carcinoma Database Consortium risk group in patients with advanced renal cell carcinoma. ESMO Open. 2023;8(3):101210. doi: 10.1016/j.esmoop.2023.101210. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
