

Coexistence of early gastric cancer and benign submucosal lesions mimic invasive cancer: a retrospective multicenter experience
- PMID: 37996821
- PMCID: PMC10666314
- DOI: 10.1186/s12876-023-03044-3
Coexistence of early gastric cancer and benign submucosal lesions mimic invasive cancer: a retrospective multicenter experience
Abstract
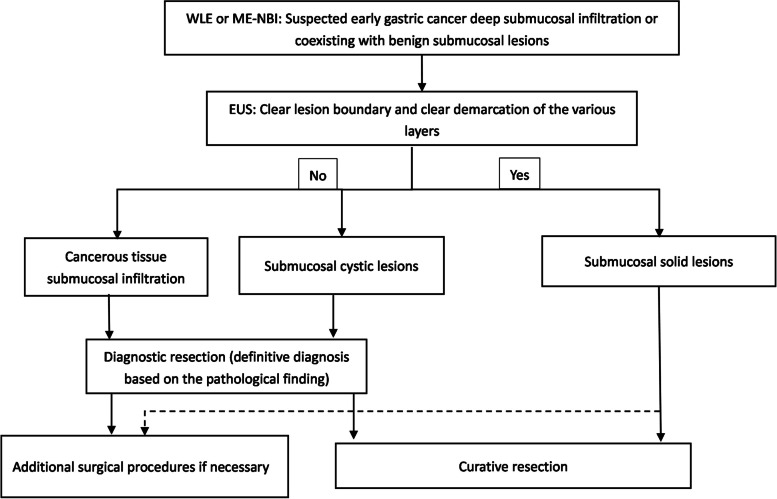
Objective: To present a study to identify the characteristics of coexisting early gastric cancer (EGC) and benign submucosal lesions, with the aim of reducing the adverse consequences of overdiagnosis and overtreatment.
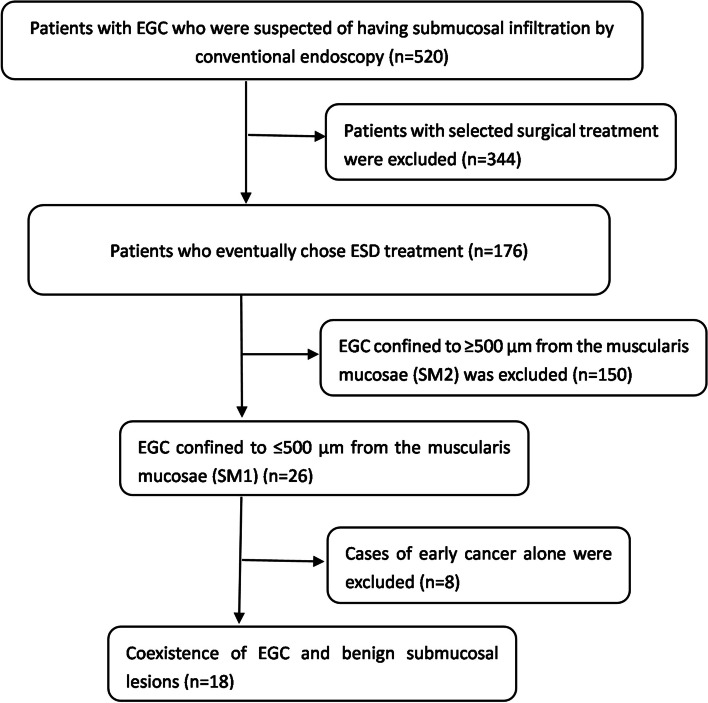
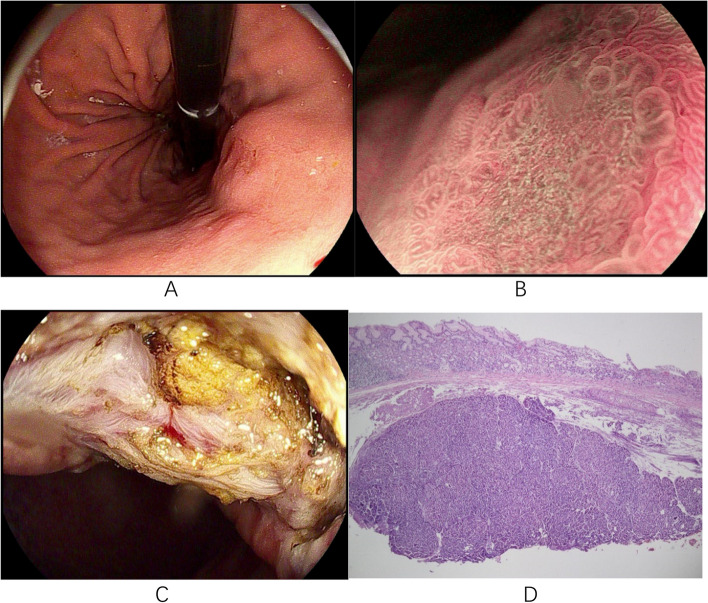
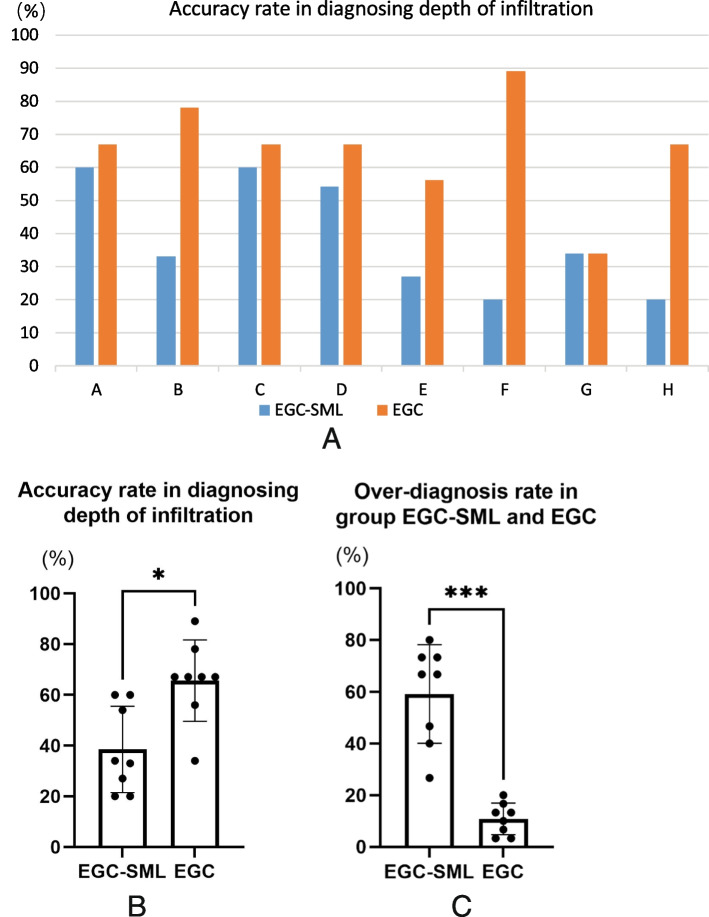
Methods: In this retrospective study, we searched the endoscopic databases of three tertiary centers. We screened of patients suspected of early gastric cancer submucosal infiltration by conventional endoscopy and ultimately selected for endoscopic submucosal dissection treatment after endoscopic ultrasonography and magnifying endoscopy with narrow-band imaging examination. Patients with coexisting EGC and benign submucosal lesions in histological sections were included. Clinical data and endoscopic images were reviewed. To evaluate the precision of endoscopists' diagnoses for this type of lesion, eight endoscopists with different experiences were recruited to judge the infiltration depth of these lesions and analyze the accuracy rate.
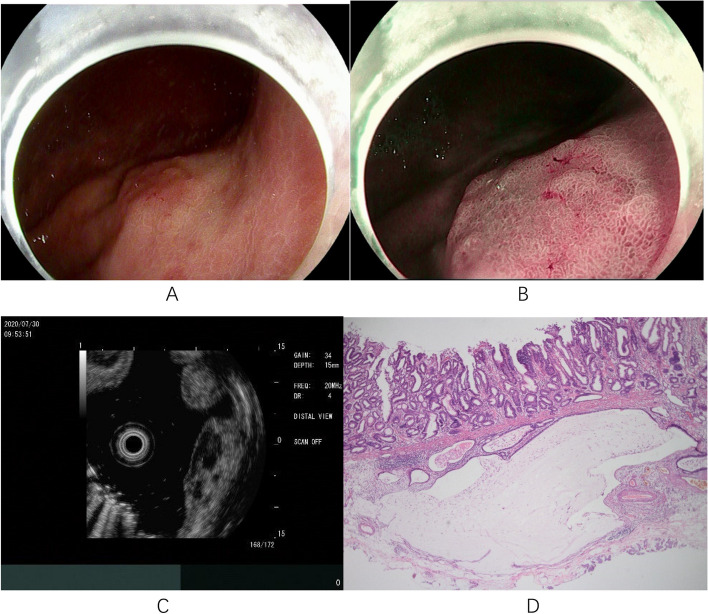
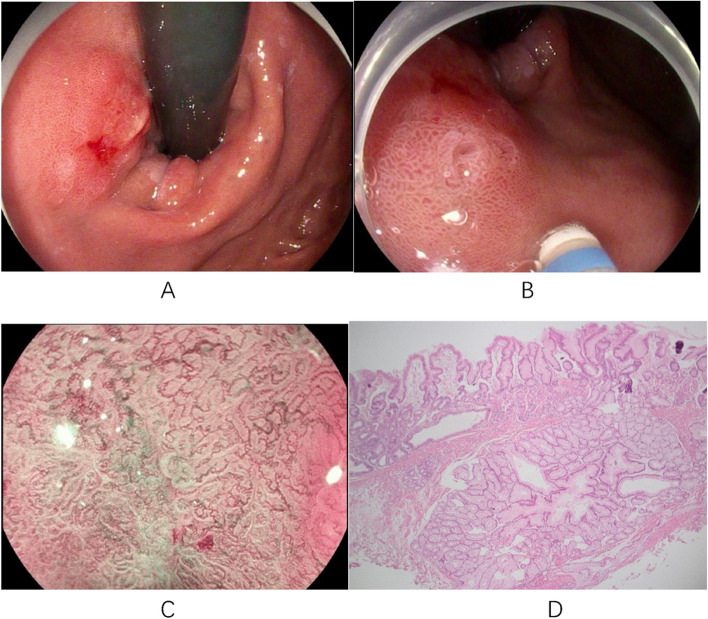
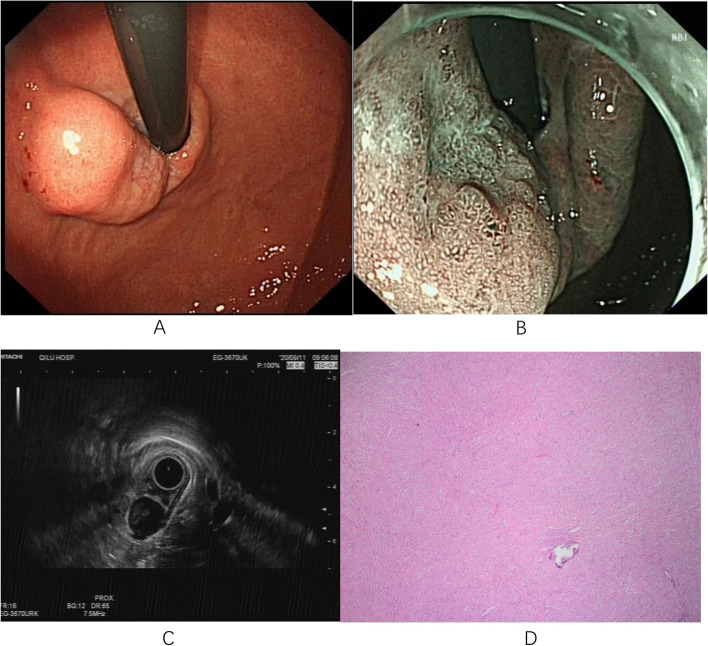
Results: We screened 520 patients and retrospectively identified 18 EGC patients with an invasive cancer-like morphology. The most common lesion site was the cardia (12/18, 66.67%). The coexisting submucosal lesions could be divided into solid (5/18, 27.78%) and cystic (13/18, 72.22%). The most common type of submucosal lesion was gastritis cystica profunda (12/18, 66.67%), whereas leiomyoma was the predominant submucosal solid lesion (3/18, 16.67%). Ten (55.56%) patients < underwent endoscopic ultrasonography; submucosal lesions were definitively diagnosed in 6 patients (60.00%). The accuracy of judgement of the infiltration depth was significantly lower in cases of coexistence of EGC with benign submucosal lesions (EGC-SML) than in EGC (38.50% versus 65.60%, P = 0.0167). The rate of over-diagnosis was significantly higher within the EGC-SML group compared to the EGC group (59.17% versus 10.83%, P < 0.0001).
Conclusions: We should be aware of the coexistence of EGC and benign submucosal lesions, the most common of which is early cardiac-differentiated cancer with gastritis cystica profunda.
Keywords: Early gastric cancer; Endoscopic ultrasonography; Gastritis cystica profunda; Infiltration depth; Submucosal lesions.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Synchronous double superficial mixed gastrointestinal mucus phenotype gastric cancer with gastritis cystica profunda and submucosal lipoma: A case report.Medicine (Baltimore). 2018 Jun;97(22):e10825. doi: 10.1097/MD.0000000000010825. Medicine (Baltimore). 2018. PMID: 29851789 Free PMC article.
-
Endoscopic features and treatments of gastric cystica profunda.World J Gastroenterol. 2024 Feb 21;30(7):673-684. doi: 10.3748/wjg.v30.i7.673. World J Gastroenterol. 2024. PMID: 38515955 Free PMC article.
-
Impact of endoscopic surveillance on the early diagnosis and endoscopic resection likelihood of gastric cancer.Surg Endosc. 2024 Apr;38(4):2188-2196. doi: 10.1007/s00464-024-10748-4. Epub 2024 Mar 6. Surg Endosc. 2024. PMID: 38448623
-
AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States.Clin Gastroenterol Hepatol. 2019 Jan;17(1):16-25.e1. doi: 10.1016/j.cgh.2018.07.041. Epub 2018 Aug 2. Clin Gastroenterol Hepatol. 2019. PMID: 30077787 Review.
-
Gastritis cystica profunda: a case report and literature review.Ann Palliat Med. 2020 Sep;9(5):3668-3677. doi: 10.21037/apm-20-1253. Ann Palliat Med. 2020. PMID: 33065804 Review.
Cited by
-
Gastric cystica profunda: Another indication for minimally invasive endoscopic resection techniques?World J Gastroenterol. 2024 Jul 21;30(27):3278-3283. doi: 10.3748/wjg.v30.i27.3278. World J Gastroenterol. 2024. PMID: 39086743 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
