

Impact of frailty on the outcomes of patients undergoing degenerative spine surgery: a systematic review and meta-analysis
- PMID: 37996826
- PMCID: PMC10668507
- DOI: 10.1186/s12877-023-04448-2
Impact of frailty on the outcomes of patients undergoing degenerative spine surgery: a systematic review and meta-analysis
Abstract
Background: Degenerative spinal diseases are common in older adults with concurrent frailty. Preoperative frailty is a strong predictor of adverse clinical outcomes after surgery. This study aimed to investigate the association between health-related outcomes and frailty in patients undergoing spine surgery for degenerative spine diseases.
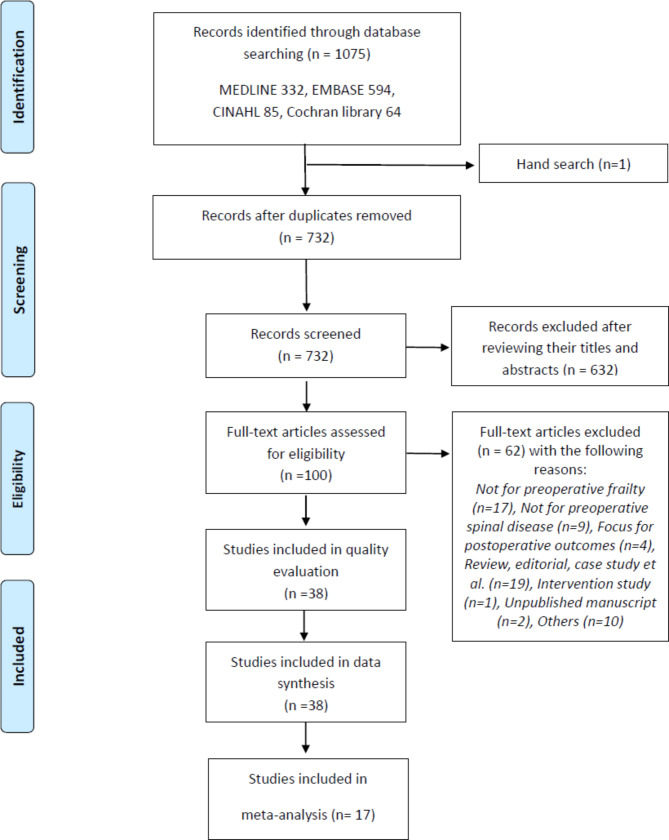
Methods: A systematic review and meta-analysis were performed by electronically searching Ovid-MEDLINE, Ovid-Embase, Cochrane Library, and CINAHL for eligible studies until July 16, 2022. We reviewed all studies, excluding spinal tumours, non-surgical procedures, and experimental studies that examined the association between preoperative frailty and related outcomes after spine surgery. A total of 1,075 articles were identified in the initial search and were reviewed by two reviewers, independently. Data were subjected to qualitative and quantitative syntheses by meta-analytic methods.
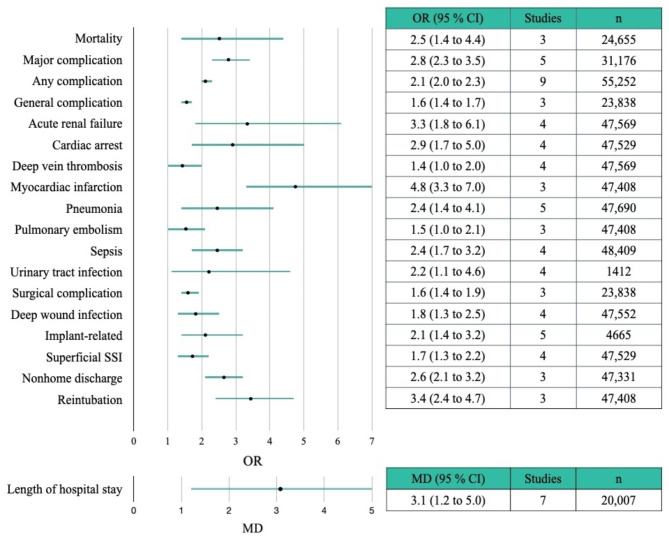
Results: Thirty-eight articles on 474,651 patients who underwent degenerative spine surgeries were included and 17 papers were quantitatively synthesized. The health-related outcomes were divided into clinical outcomes and patient-reported outcomes; clinical outcomes were further divided into postoperative complications and supportive management procedures. Compared to the non-frail group, the frail group was significantly associated with a greater risk of high mortality, major complications, acute renal failure, myocardial infarction, non-home discharge, reintubation, and longer length of hospital stay. Regarding patient-reported outcomes, changes in scores between the preoperative and postoperative Oswestry Disability Index scores were not associated with preoperative frailty.
Conclusions: In degenerative spinal diseases, frailty is a strong predictor of adverse clinical outcomes after spine surgery. The relationship between preoperative frailty and patient-reported outcomes is still inconclusive. Further research is needed to consolidate the evidence from patient-reported outcomes.
Keywords: Frailty; Meta-analysis; Patient-reported outcome measures; Spine surgery; Systematic review.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
