

Effect of different cement distribution in bilateral and unilateral Percutaneous vertebro plasty on the clinical efficacy of vertebral compression fractures
- PMID: 37996830
- PMCID: PMC10666391
- DOI: 10.1186/s12891-023-06997-4
Effect of different cement distribution in bilateral and unilateral Percutaneous vertebro plasty on the clinical efficacy of vertebral compression fractures
Abstract
Background: The ramifications of osteoporotic fractures and their subsequent complications are becoming progressively detrimental for the elderly population. This study evaluates the clinical ramifications of postoperative bone cement distribution in patients with osteoporotic vertebral compression fractures (OVCF) who underwent both bilateral and unilateral Percutaneous Vertebroplasty (PVP).
Objective: The research aims to discern the influence of bone cement distribution on the clinical outcomes of both bilateral and unilateral Percutaneous Vertebroplasty. The overarching intention is to foster efficacious preventive and therapeutic strategies to mitigate postoperative vertebral fractures and thereby enhance surgical outcomes.
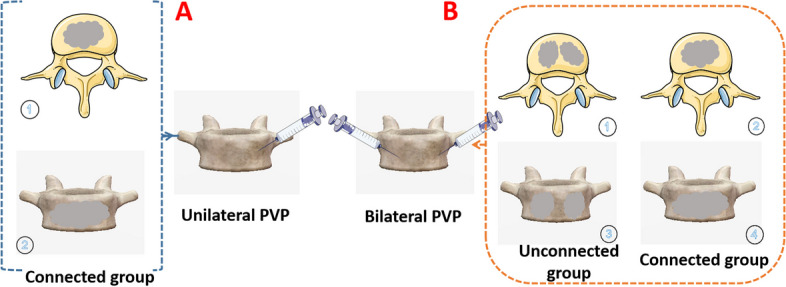
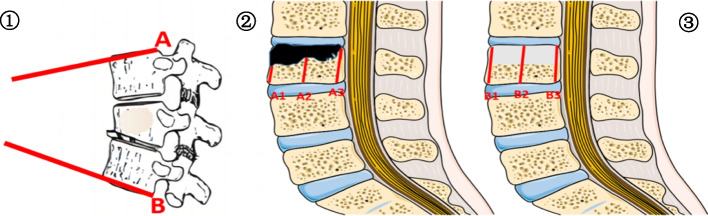
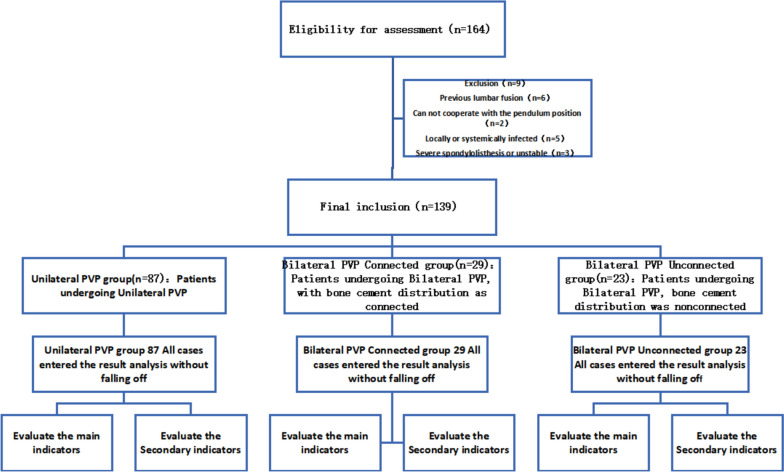
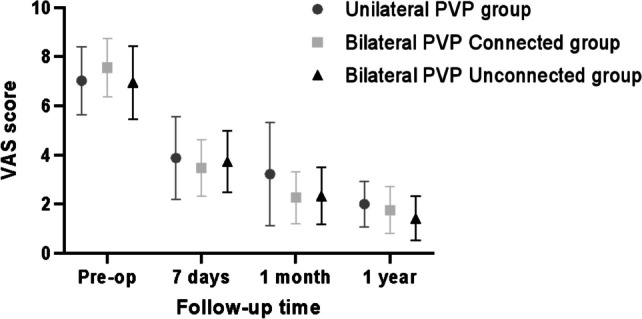
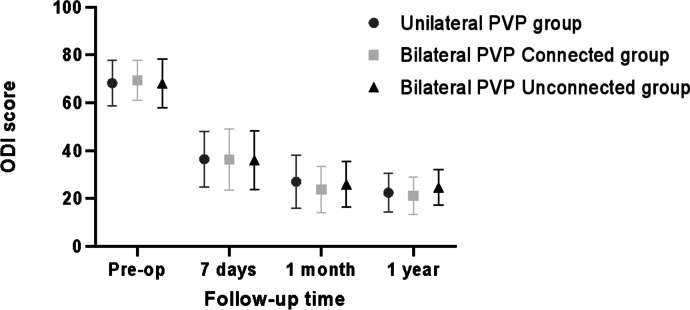
Methods: A comprehensive evaluation was undertaken on 139 patients who received either bilateral or unilateral PVP in our institution between January 2018 and March 2022. These patients were systematically classified into three distinct groups: unilateral PVP (n = 87), bilateral PVP with a connected modality (n = 29), and bilateral PVP with a disconnected modality (n = 23). Several operational metrics were juxtaposed across these cohorts, encapsulating operative duration, aggregate hospital expenses, bone cement administration metrics, VAS (Visual Analogue Scale) scores, ODI (Oswestry Disability Index) scores relative to lumbar discomfort, postoperative vertebral height restitution rates, and the status of the traumatized and adjacent vertebral bodies. Preliminary findings indicated that the VAS scores for the January and December cohorts were considerably reduced compared to the unilateral PVP group (P = 0.015, 0.032). Furthermore, the recurrence of fractures in the affected and adjacent vertebral structures was more pronounced in the unilateral PVP cohort compared to the bilateral PVP cohorts. The duration of the procedure (P = 0.000) and the overall hospitalization expenses for the unilateral PVP group were markedly lesser than for both the connected and disconnected bilateral PVP groups, a difference that was statistically significant (P = 0.015, P = 0.024, respectively). Nevertheless, other parameters, such as the volume of cement infused, incidence of cement spillage, ODI scores for lumbar discomfort, post-surgical vertebral height restitution rate, localized vertebral kyphosis, and the alignment of cement and endplate, did not exhibit significant statistical deviations (P > 0.05).
Conclusion: In juxtaposition with unilateral PVP, the employment of bilateral PVP exhibits enhanced long-term prognostic outcomes for patients afflicted with vertebral compression fractures. Notably, bilateral PVP significantly curtails the prevalence of subsequent vertebral injuries. Conversely, the unilateral PVP cohort is distinguished by its abbreviated operational duration, minimal invasiveness, and reduced overall hospitalization expenditures, conferring it with substantial clinical applicability and merit.
Keywords: Bone cement; Bone cement distribution; Osteoporotic vertebral compression fracture; Percutaneous vertebro plasty.
© 2023. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Similar articles
-
[COMPARISON OF EFFECTIVENESS BETWEEN PERCUTANEOUS VERTEBROPLASTY AND PERCUTANEOUS KYPHOPLASTY FOR TREATMENT OF OSTEOPOROTIC VERTEBRAL COMPRESSION FRACTURE WITH INTRAVERTEBRAL VACUUM CLEFT].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016 Sep 8;30(9):1104-1110. doi: 10.7507/1002-1892.20160225. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016. PMID: 29786364 Chinese.
-
Two different unilateral percutaneous vertebroplasty approaches for acute osteoporotic vertebral compression fractures: clinical and radiological outcomes.BMC Musculoskelet Disord. 2025 Jul 4;26(1):628. doi: 10.1186/s12891-025-08887-3. BMC Musculoskelet Disord. 2025. PMID: 40615843 Free PMC article.
-
[Application of Curved Diffusion Needle in unilateral percutaneous vertebroplasty].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021 Dec 15;35(12):1587-1594. doi: 10.7507/1002-1892.202107044. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021. PMID: 34913316 Free PMC article. Chinese.
-
Effect of different cement distribution on the clinical efficacy of vertebral compression fractures in unilateral percutaneous vertebroplasty.Eur Spine J. 2025 May;34(5):1673-1684. doi: 10.1007/s00586-024-08630-x. Epub 2025 Feb 13. Eur Spine J. 2025. PMID: 39945854 Review.
-
Comparison of Percutaneous Vertebroplasty and Balloon Kyphoplasty for the Treatment of Single Level Vertebral Compression Fractures: A Meta-analysis of the Literature.Pain Physician. 2015 May-Jun;18(3):209-22. Pain Physician. 2015. PMID: 26000665 Review.
Cited by
-
Comparison of the efficacy of bilateral approach PVP and lateral hole injection combined with modified fluoroscopic unilateral approach PVP in the treatment of thoracolumbar osteoporotic fractures.BMC Surg. 2025 Jul 3;25(1):263. doi: 10.1186/s12893-025-02985-8. BMC Surg. 2025. PMID: 40611119 Free PMC article.
-
Clinical effect analysis of unilateral percutaneous vertebral cement distribution in the repair of osteoporotic thoracolumbar vertebral compression fractures.BMC Surg. 2025 Mar 5;25(1):90. doi: 10.1186/s12893-025-02820-0. BMC Surg. 2025. PMID: 40045301 Free PMC article.
-
Risk factors for different cement distribution indexes for refracture of operated vertebrae and adjacent vertebrae after percutaneous vertebroplasty in patients with thoracolumbar compression fracture.BMC Surg. 2025 Jul 19;25(1):306. doi: 10.1186/s12893-025-03033-1. BMC Surg. 2025. PMID: 40682022 Free PMC article.
-
Biomechanical study between percutaneous vertebroplasty combined with cement pedicle plasty improves vertebral biomechanical stability: A finite element analysis.BMC Musculoskelet Disord. 2024 Jul 29;25(1):597. doi: 10.1186/s12891-024-07689-3. BMC Musculoskelet Disord. 2024. PMID: 39075431 Free PMC article.
-
Bone cement distribution patterns in vertebral augmentation for osteoporotic vertebral compression fractures: a systematic review.J Orthop Surg Res. 2025 Jun 4;20(1):568. doi: 10.1186/s13018-025-05868-z. J Orthop Surg Res. 2025. PMID: 40468349 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
