

Perioperative predictive factors of failure to rescue following highly advanced hepatobiliary-pancreatic surgery: a single-institution retrospective study
- PMID: 37996865
- PMCID: PMC10668400
- DOI: 10.1186/s12957-023-03257-6
Perioperative predictive factors of failure to rescue following highly advanced hepatobiliary-pancreatic surgery: a single-institution retrospective study
Abstract
Background: Failure to rescue (FTR), defined as a postoperative complication leading to death, is a recently described outcome metric used to evaluate treatment quality. However, the predictive factors for FTR, particularly following highly advanced hepatobiliary-pancreatic surgery (HBPS), have not been adequately investigated. This study aimed to identify perioperative predictive factors for FTR following highly advanced HBPS.
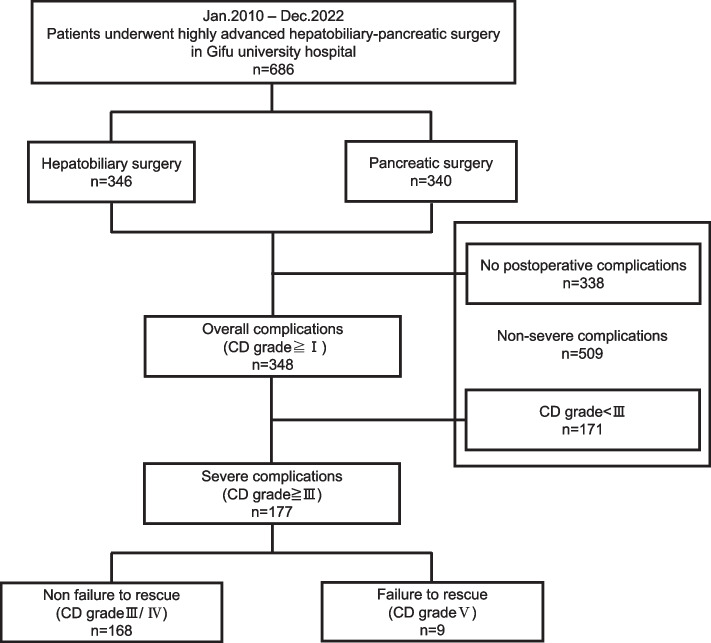
Methods: This single-institution retrospective study involved 177 patients at Gifu University Hospital, Japan, who developed severe postoperative complications (Clavien-Dindo classification grades ≥ III) between 2010 and 2022 following highly advanced HBPS. Univariate analysis was used to identify pre-, intra-, and postoperative risks of FTR.
Results: Nine postoperative mortalities occurred during the study period (overall mortality rate, 1.3% [9/686]; FTR rate, 5.1% [9/177]). Univariate analysis indicated that comorbid liver disease, intraoperative blood loss, intraoperative blood transfusion, postoperative liver failure, postoperative respiratory failure, and postoperative bleeding significantly correlated with FTR.
Conclusions: FTR was found to be associated with perioperative factors. Well-coordinated surgical procedures to avoid intra- and postoperative bleeding and unnecessary blood transfusions, as well as postoperative team management with attention to the occurrence of organ failure, may decrease FTR rates.
Keywords: Failure to rescue; Highly advanced hepatobiliary-pancreatic surgery; Perioperative predictive factors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Similar articles
-
Failure to rescue as a source of variation in hospital mortality after rectal surgery: The Italian experience.Eur J Surg Oncol. 2019 Jul;45(7):1219-1224. doi: 10.1016/j.ejso.2019.03.006. Epub 2019 Mar 16. Eur J Surg Oncol. 2019. PMID: 30904244
-
Failure to rescue after major abdominal surgery: The role of hospital safety net burden.Am J Surg. 2020 Oct;220(4):1023-1030. doi: 10.1016/j.amjsurg.2020.03.014. Epub 2020 Mar 12. Am J Surg. 2020. PMID: 32199603
-
Impact of Sarcopenic Obesity on Failure to Rescue from Major Complications Following Pancreaticoduodenectomy for Cancer: Results from a Multicenter Study.Ann Surg Oncol. 2018 Jan;25(1):308-317. doi: 10.1245/s10434-017-6216-5. Epub 2017 Nov 7. Ann Surg Oncol. 2018. PMID: 29116490
-
Failure to rescue in the surgical patient: a review.Curr Opin Crit Care. 2019 Dec;25(6):706-711. doi: 10.1097/MCC.0000000000000667. Curr Opin Crit Care. 2019. PMID: 31567517 Review.
-
Variation in the definition of 'failure to rescue' from postoperative complications: a systematic review and recommendations for outcome reporting.Surgery. 2024 Apr;175(4):1103-1110. doi: 10.1016/j.surg.2023.12.006. Epub 2024 Jan 19. Surgery. 2024. PMID: 38245447
Cited by
-
Postoperative C-reactive protein to albumin ratio as early predictive factors for prolonged postoperative hospital stay after highly advanced hepatobiliary-pancreatic surgery: a single-center retrospective study.BMC Surg. 2025 Aug 23;25(1):387. doi: 10.1186/s12893-025-03112-3. BMC Surg. 2025. PMID: 40849630 Free PMC article.
References
-
- van Rijssen LB, Zwart MJ, van Dieren S, de Rooij T, Bonsing BA, Bosscha K, et al. Variation in hospital mortality after pancreatoduodenectomy is related to failure to rescue rather than major complications: a nationwide audit. HPB (Oxford) 2018;20:759–767. doi: 10.1016/j.hpb.2018.02.640. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
