

Protection Conferred by COVID-19 Vaccination, Prior SARS-CoV-2 Infection, or Hybrid Immunity Against Omicron-Associated Severe Outcomes Among Community-Dwelling Adults
- PMID: 38001037
- PMCID: PMC11093681
- DOI: 10.1093/cid/ciad716
Protection Conferred by COVID-19 Vaccination, Prior SARS-CoV-2 Infection, or Hybrid Immunity Against Omicron-Associated Severe Outcomes Among Community-Dwelling Adults
Abstract
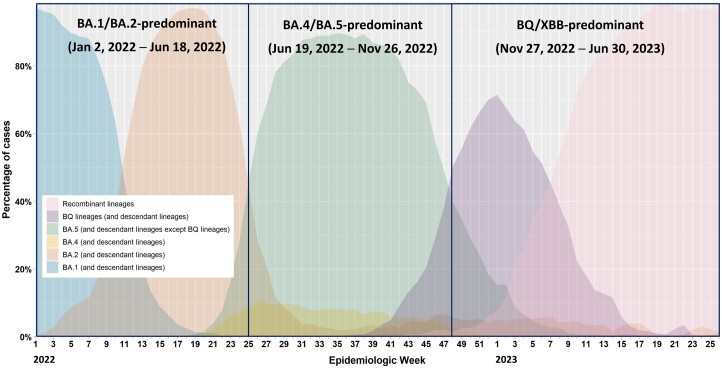
Introduction: We assessed protection from coronavirus disease 2019 (COVID-19) vaccines and/or prior severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection against Omicron-associated severe outcomes during successive sublineage-predominant periods.
Methods: We used a test-negative design to estimate protection by vaccines and/or prior infection against hospitalization/death among community-dwelling, polymerase chain reaction (PCR)-tested adults aged ≥50 years in Ontario, Canada, between 2 January 2022 and 30 June 2023. Multivariable logistic regression was used to estimate the relative change in the odds of hospitalization/death with each vaccine dose (2-5) and/or prior PCR-confirmed SARS-CoV-2 infection (compared with unvaccinated, uninfected subjects) up to 15 months since the last vaccination or infection.
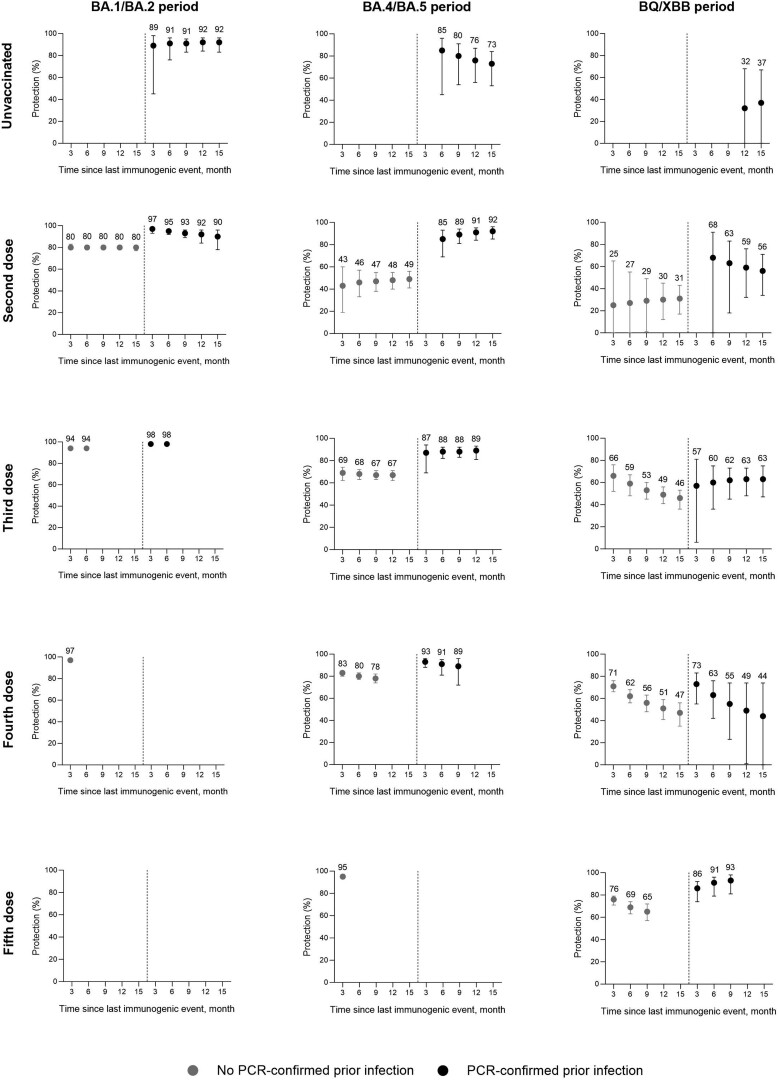
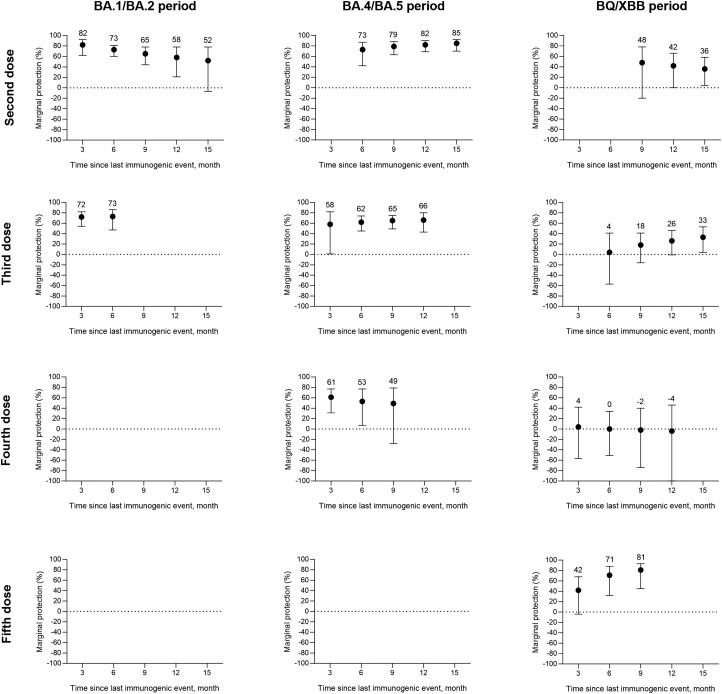
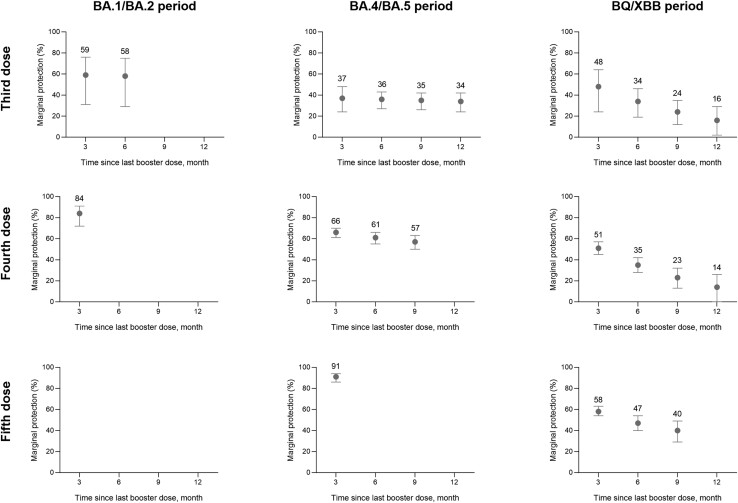
Results: We included 18 526 cases with Omicron-associated severe outcomes and 90 778 test-negative controls. Vaccine protection was high during BA.1/BA.2 predominance but was generally <50% during periods of BA.4/BA.5 and BQ/XBB predominance without boosters. A third/fourth dose transiently increased protection during BA.4/BA.5 predominance (third-dose, 6-month: 68%, 95% confidence interval [CI] 63%-72%; fourth-dose, 6-month: 80%, 95% CI 77%-83%) but was lower and waned quickly during BQ/XBB predominance (third-dose, 6-month: 59%, 95% CI 48%-67%; 12-month: 49%, 95% CI 41%-56%; fourth-dose, 6-month: 62%, 95% CI 56%-68%, 12-months: 51%, 95% CI 41%-56%). Hybrid immunity conferred nearly 90% protection throughout BA.1/BA.2 and BA.4/BA.5 predominance but was reduced during BQ/XBB predominance (third-dose, 6-month: 60%, 95% CI 36%-75%; fourth-dose, 6-month: 63%, 95% CI 42%-76%). Protection was restored with a fifth dose (bivalent; 6-month: 91%, 95% CI 79%-96%). Prior infection alone did not confer lasting protection.
Conclusions: Protection from COVID-19 vaccines and/or prior SARS-CoV-2 infections against severe outcomes is reduced when immune-evasive variants/subvariants emerge and may also wane over time. Our findings support a variant-adapted booster vaccination strategy with periodic review.
Keywords: COVID-19 vaccination; Omicron; adults; hybrid immunity; severe outcomes.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. N. L. has previously received honoraria for consultancy work, speaking in educational programs, and/or travel support from: Shionogi Inc., Gilead Sciences Canada Inc., Janssen Inc., GlaxoSmithKline plc., Sanofi Pasteur Ltd., F. Hoffmann-La Roche Ltd., Genentech Inc., CIDARA Therapeutics Inc., Clarion Healthcare, bioStrategies, Technospert, Aligos; all unrelated to this work. K. W. is a shareholder and board member and Co-founder and Chief Scientific Officer of CANImmunize Inc. and has served on independent scientific advisory boards for Medicago (Independent Data Monitoring Committee) and Moderna (Global Advisory Core Consultancy Group). J. G. reports a position as a paid consultant scientific editor for GIDEON Informatics, Inc., which is unrelated to the current work. S. E. W. reports being a co-investigator on a grant related to public health surveillance of invasive pneumococcal disease (no involvement in administration of funds) for the Canadian Immunization Research Network and a co-investigator on a grant on immunization data in Canada (no involvement in administration of funds) for CIRN; travel support to attend the Future of Vaccinology conference in October 2023 as an invited speaker from McMaster University (Hamilton, ON) and a role as an unpaid volunteer member for Canada's National Advisory Committee on Immunization (NACI). All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Similar articles
-
Limited durability of protection conferred by XBB.1.5 vaccines against omicron-associated severe outcomes among community-dwelling adults, Ontario, Canada.Vaccine. 2025 Jul 11;60:127300. doi: 10.1016/j.vaccine.2025.127300. Epub 2025 May 26. Vaccine. 2025. PMID: 40424706
-
BNT162b2 vaccine protection against omicron and effect of previous infection variant and vaccination sequence among children and adolescents in Singapore: a population-based cohort study.Lancet Child Adolesc Health. 2023 Jul;7(7):463-470. doi: 10.1016/S2352-4642(23)00101-3. Epub 2023 May 15. Lancet Child Adolesc Health. 2023. PMID: 37201540 Free PMC article.
-
Protective immunity of SARS-CoV-2 infection and vaccines against medically attended symptomatic omicron BA.4, BA.5, and XBB reinfections in Singapore: a national cohort study.Lancet Infect Dis. 2023 Jul;23(7):799-805. doi: 10.1016/S1473-3099(23)00060-9. Epub 2023 Mar 13. Lancet Infect Dis. 2023. PMID: 36924786 Free PMC article.
-
Real-world evidence on the efficacy of bivalent booster doses of SARS-CoV-2 vaccine in respect of monovalent boosters or primary cycle of vaccination: a narrative review.Epidemiol Prev. 2023 Nov-Dec;47(6):331-343. doi: 10.19191/EP23.6.A626.081. Epidemiol Prev. 2023. PMID: 38314543 Review. English.
-
Protection of the third-dose and fourth-dose mRNA vaccines against SARS-CoV-2 Omicron subvariant: a systematic review and meta-analysis.BMJ Open. 2023 Dec 20;13(12):e076892. doi: 10.1136/bmjopen-2023-076892. BMJ Open. 2023. PMID: 38128943 Free PMC article.
Cited by
-
Vaccine Effectiveness against GP-Attended Symptomatic COVID-19 and Hybrid Immunity among Adults in Hungary during the 2022-2023 Respiratory Season Dominated by Different SARS-CoV-2 Omicron Subvariants.Vaccines (Basel). 2024 May 4;12(5):496. doi: 10.3390/vaccines12050496. Vaccines (Basel). 2024. PMID: 38793747 Free PMC article.
-
Effectiveness of the fourth dose of COVID-19 vaccines against severe COVID-19 among adults 40 years or older in Brazil: a population-based cohort study.Lancet Reg Health Am. 2024 May 3;34:100755. doi: 10.1016/j.lana.2024.100755. eCollection 2024 Jun. Lancet Reg Health Am. 2024. PMID: 38737773 Free PMC article.
-
Comparison of two methods for the estimation of COVID-19 vaccine effectiveness of the autumnal booster within the VEBIS-EHR network in 2022/23.Epidemiol Infect. 2025 Mar 17;153:e54. doi: 10.1017/S0950268825000317. Epidemiol Infect. 2025. PMID: 40090768 Free PMC article.
-
Situation Analysis of Immune Response Status One Year After the Nationwide COVID-19 Vaccination in Cameroon: Role of Obesity and SARS-CoV-2 Infection.Health Sci Rep. 2025 Jul 18;8(7):e71068. doi: 10.1002/hsr2.71068. eCollection 2025 Jul. Health Sci Rep. 2025. PMID: 40687548 Free PMC article.
-
Predictors of moderate, severe, and critical COVID-19 infection in a largely vaccinated kidney transplant recipient cohort during the Omicron era: the importance of timely booster vaccinations and early presentation to care.Clin Transplant Res. 2025 Mar 31;39(1):46-54. doi: 10.4285/ctr.24.0045. Epub 2025 Feb 6. Clin Transplant Res. 2025. PMID: 39909823 Free PMC article.
References
-
- UK Health and Security Agency . COVID-19 vaccine monthly surveillance reports (week 39 2021 to week 14 2023). Available at: https://www.gov.uk/government/publications/covid-19-vaccine-weekly-surve.... Accessed 15 August 2023.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
