

Low-dose radiotherapy combined with dual PD-L1 and VEGFA blockade elicits antitumor response in hepatocellular carcinoma mediated by activated intratumoral CD8+ exhausted-like T cells
- PMID: 38001101
- PMCID: PMC10673920
- DOI: 10.1038/s41467-023-43462-1
Low-dose radiotherapy combined with dual PD-L1 and VEGFA blockade elicits antitumor response in hepatocellular carcinoma mediated by activated intratumoral CD8+ exhausted-like T cells
Abstract
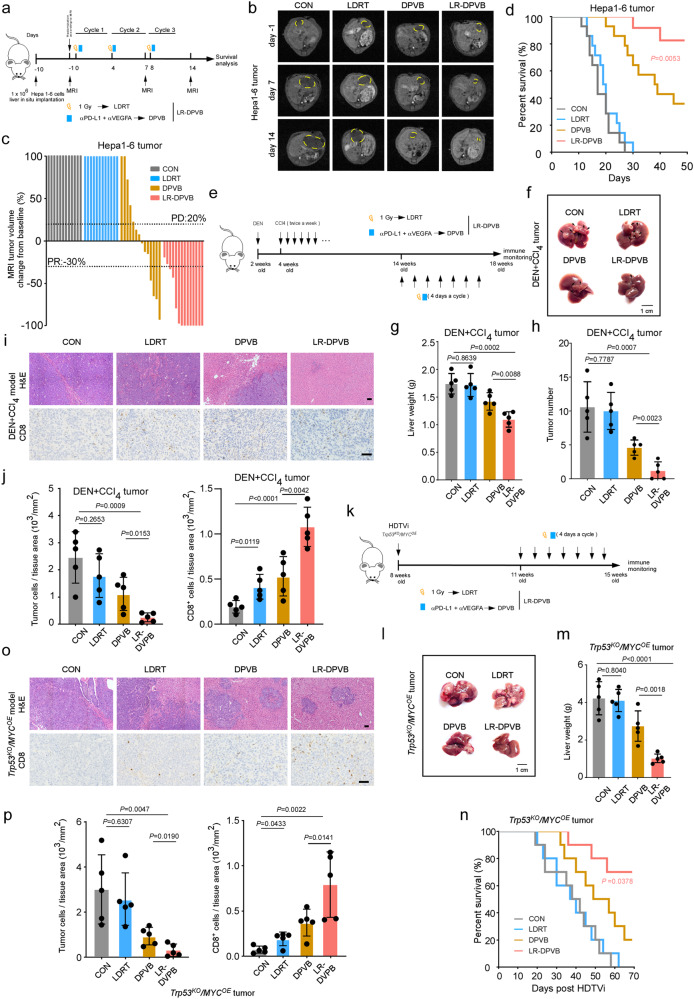
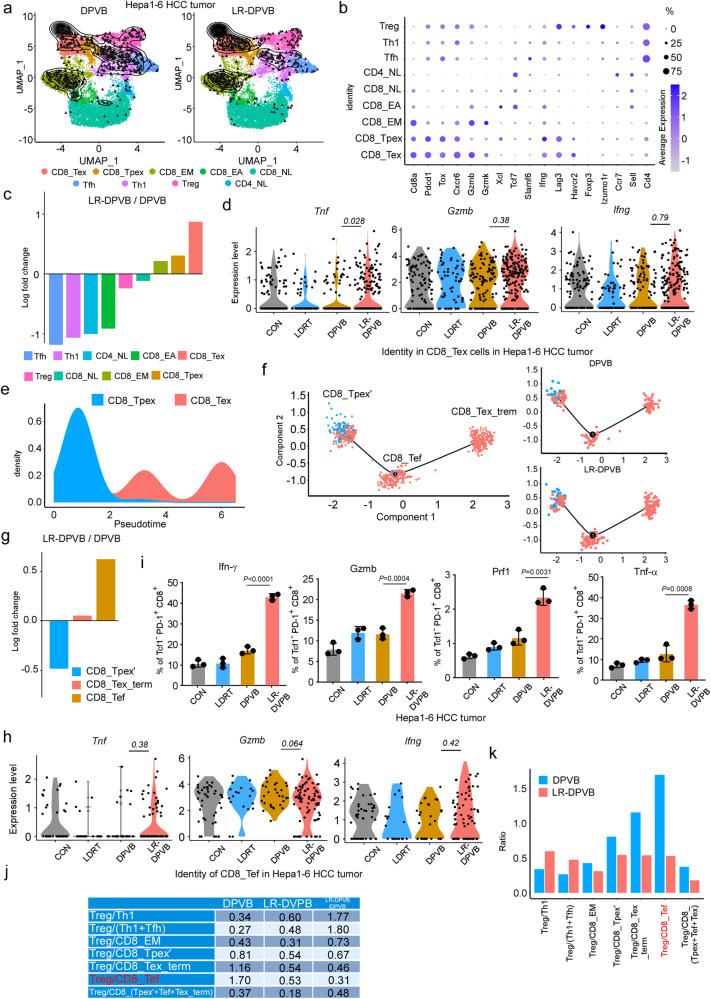
Atezolizumab (anti-PD-L1) combined with bevacizumab (anti-VEGFA) is the first-line immunotherapy for advanced hepatocellular carcinoma (HCC), but the number of patients who benefit from this regimen remains limited. Here, we combine dual PD-L1 and VEGFA blockade (DPVB) with low-dose radiotherapy (LDRT), which rapidly inflames tumors, rendering them vulnerable to immunotherapy. The combinatorial therapy exhibits superior antitumor efficacy mediated by CD8+ T cells in various preclinical HCC models. Treatment efficacy relies upon mobilizing exhausted-like CD8+ T cells (CD8+ Tex) with effector function and cytolytic capacity. Mechanistically, LDRT sensitizes tumors to DPVB by recruiting stem-like CD8+ Tpex, the progenitor exhausted CD8+ T cells, from draining lymph nodes (dLNs) into the tumor via the CXCL10/CXCR3 axis. Together, these results further support the rationale for combining LDRT with atezolizumab and bevacizumab, and its clinical translation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
- 82103448/National Natural Science Foundation of China (National Science Foundation of China)
- 82172585/National Natural Science Foundation of China (National Science Foundation of China)
- 82270688/National Natural Science Foundation of China (National Science Foundation of China)
- 81972286/National Natural Science Foundation of China (National Science Foundation of China)
- 2023A1515010322/Natural Science Foundation of Guangdong Province (Guangdong Natural Science Foundation)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
