

Development and validation of a nomogram for predicting in-hospital mortality in patients with nonhip femoral fractures
- PMID: 38001553
- PMCID: PMC10668411
- DOI: 10.1186/s40001-023-01515-7
Development and validation of a nomogram for predicting in-hospital mortality in patients with nonhip femoral fractures
Abstract
Background: The incidence of nonhip femoral fractures is gradually increasing, but few studies have explored the risk factors for in-hospital death in patients with nonhip femoral fractures in the ICU or developed mortality prediction models. Therefore, we chose to study this specific patient group, hoping to help clinicians improve the prognosis of patients.
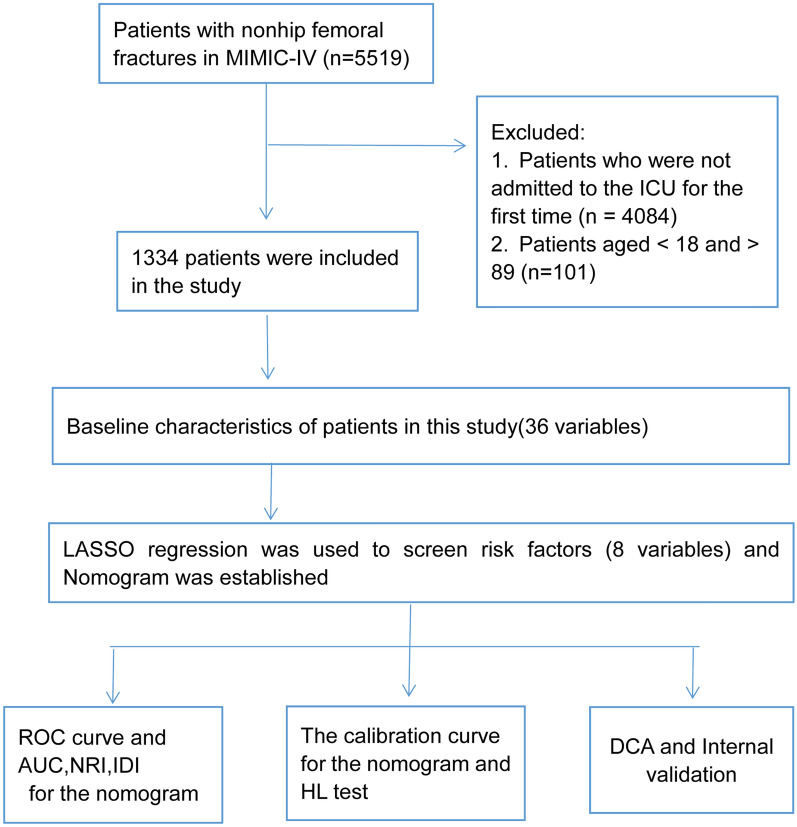
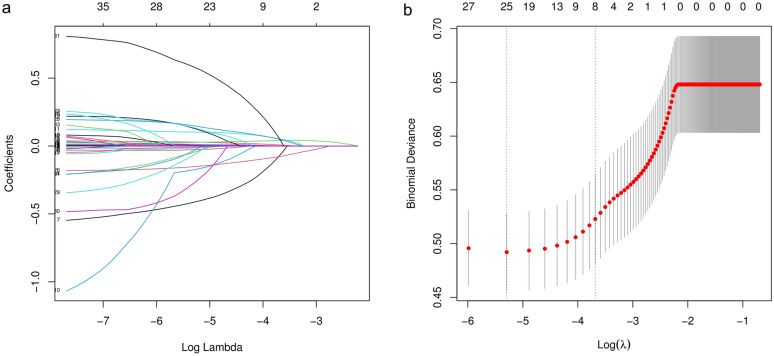
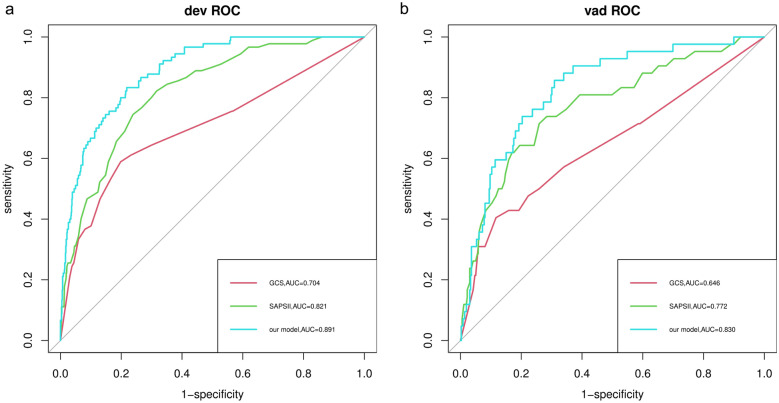
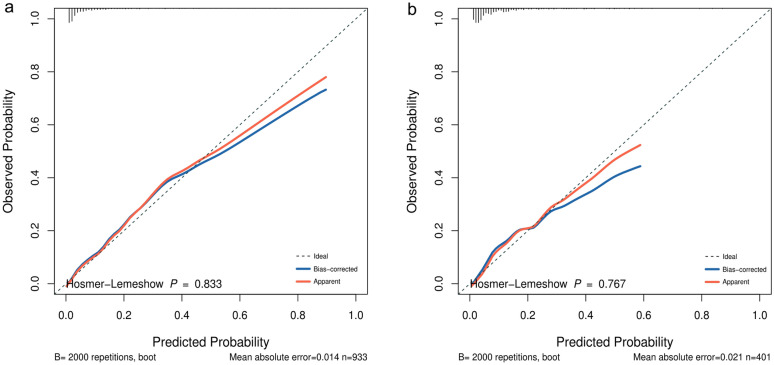
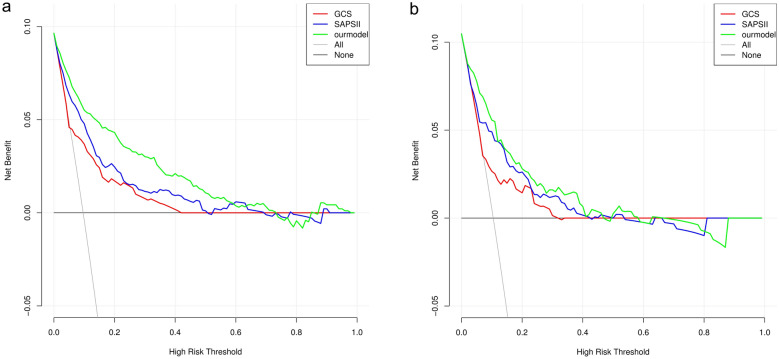
Methods: This is a retrospective study based on the data from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. Least absolute shrinkage and selection operator (LASSO) regression was used to screen risk factors. The receiver operating characteristic (ROC) curve was drawn, and the areas under the curve (AUC), net reclassification index (NRI) and integrated discrimination improvement (IDI) were calculated to evaluate the discrimination of the model. The consistency between the actual probability and the predicted probability was assessed by the calibration curve and Hosmer-Lemeshow goodness of fit test (HL test). Decision curve analysis (DCA) was performed, and the nomogram was compared with the scoring system commonly used in clinical practice to evaluate the clinical net benefit.
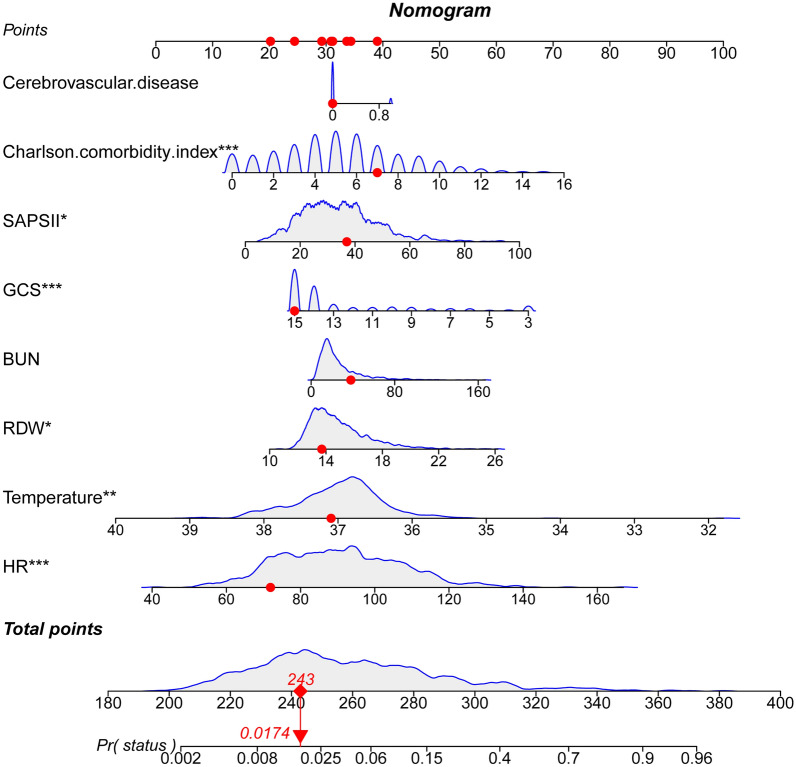
Results: The LASSO regression analysis showed that heart rate, temperature, red blood cell distribution width, blood urea nitrogen, Glasgow Coma Scale (GCS), Simplified Acute Physiology Score II (SAPSII), Charlson comorbidity index and cerebrovascular disease were independent risk factors for in-hospital death in patients with nonhip femoral fractures. The AUC, IDI and NRI of our model in the training set and validation set were better than those of the GCS and SAPSII scoring systems. The calibration curve and HL test results showed that our model prediction results were in good agreement with the actual results (P = 0.833 for the HL test of the training set and P = 0.767 for the HL test of the validation set). DCA showed that our model had a better clinical net benefit than the GCS and SAPSII scoring systems.
Conclusion: In this study, the independent risk factors for in-hospital death in patients with nonhip femoral fractures were determined, and a prediction model was constructed. The results of this study may help to improve the clinical prognosis of patients with nonhip femoral fractures.
Keywords: In-hospital mortality; Intensive care unit; Nomogram; Nonhip femoral fracture.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Development and validation of a nomogram for predicting in-hospital mortality of patients with cervical spine fractures without spinal cord injury.Eur J Med Res. 2024 Jan 29;29(1):80. doi: 10.1186/s40001-024-01655-4. Eur J Med Res. 2024. PMID: 38287435 Free PMC article.
-
Nomogram predictive model for in-hospital mortality risk in elderly ICU patients with urosepsis.BMC Infect Dis. 2024 Apr 26;24(1):442. doi: 10.1186/s12879-024-09319-8. BMC Infect Dis. 2024. PMID: 38671376 Free PMC article.
-
Development and Internal Validation of a Nomogram to Predict Mortality During the ICU Stay of Thoracic Fracture Patients Without Neurological Compromise: An Analysis of the MIMIC-III Clinical Database.Front Public Health. 2021 Dec 22;9:818439. doi: 10.3389/fpubh.2021.818439. eCollection 2021. Front Public Health. 2021. PMID: 35004604 Free PMC article.
-
Predictive nomogram for 28-day mortality risk in mitral valve disorder patients in the intensive care unit: A comprehensive assessment from the MIMIC-III database.Int J Cardiol. 2024 Jul 15;407:132105. doi: 10.1016/j.ijcard.2024.132105. Epub 2024 Apr 25. Int J Cardiol. 2024. PMID: 38677334
-
Suggestions for designing studies investigating diagnostic accuracy of biomarkers.Ann Transl Med. 2019 Dec;7(23):788. doi: 10.21037/atm.2019.11.133. Ann Transl Med. 2019. PMID: 32042804 Free PMC article. Review.
References
-
- Knauf T, Jensen KO, Hack J, Barthel J, Althaus H, Buecking B, Aigner R, Knobe M, Ruchholtz S, Eschbach D. Type of underlying fracture after the surgical treatment of geriatric trauma patients has no effect on mortality during intensive care treatment. Geriatr Gerontol Int. 2020;20(12):1120–1125. doi: 10.1111/ggi.14053. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
