

Comparison of Single-Port Laparoscopy with Other Surgical Approaches in Endometrial Cancer Surgical Staging: Propensity-Score-Matched Analysis
- PMID: 38001582
- PMCID: PMC10670050
- DOI: 10.3390/cancers15225322
Comparison of Single-Port Laparoscopy with Other Surgical Approaches in Endometrial Cancer Surgical Staging: Propensity-Score-Matched Analysis
Abstract
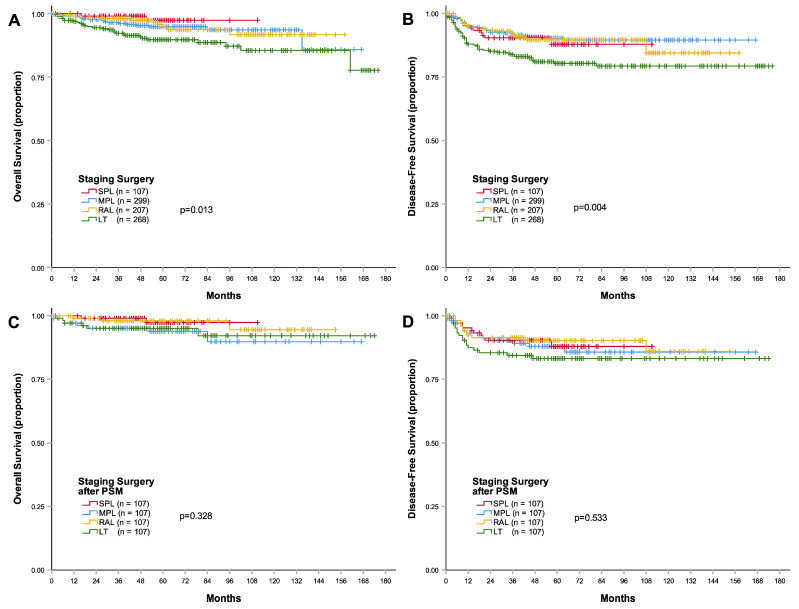
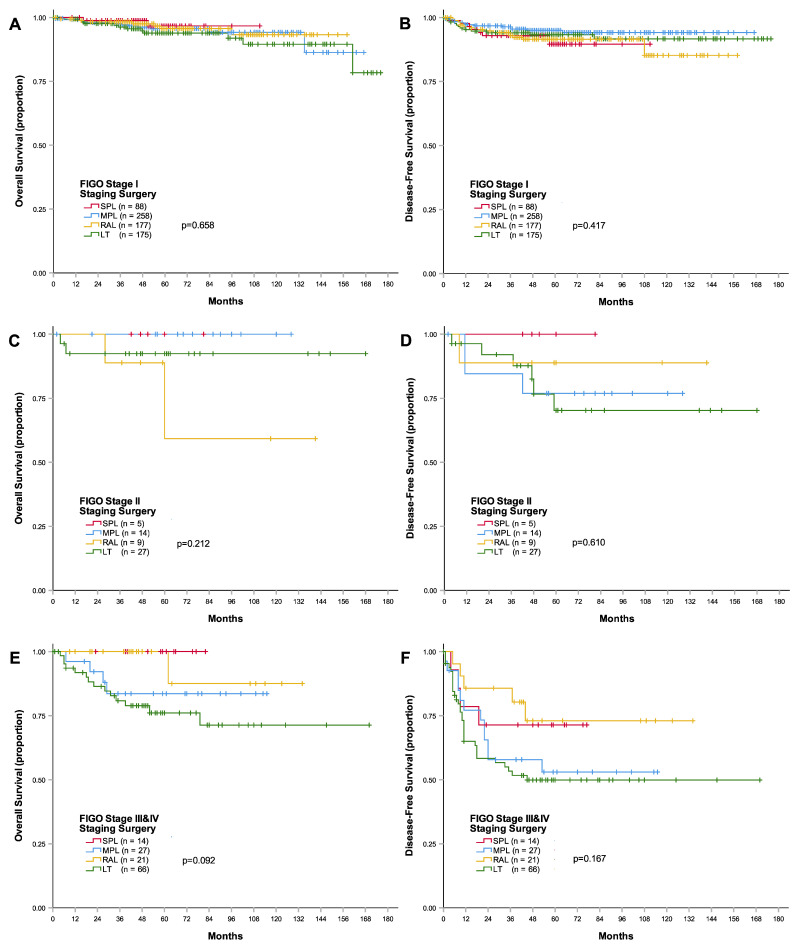
This single-institution, retrospective study aimed to compare the surgical outcomes of single-port, multi-port, and robot-assisted laparoscopy, as well as laparotomy, in patients with endometrial cancer who underwent surgical staging between January 2006 and December 2017. This study evaluated various parameters, including disease-free survival (DFS), overall survival (OS), recurrence rate (RR), recurrence site, and intra- and postoperative complications. Propensity score matching was performed to account for baseline characteristics, and a total of 881 patients were included in the analysis. The 3-year DFS of single-port laparoscopy was similar to that of the other groups, but laparotomy exhibited a lower 3-year DFS compared to multi-port (p = 0.001) and robot-assisted (p = 0.031) laparoscopy. Single-port laparoscopy resulted in a significantly higher 3-year OS than laparotomy (p = 0.013). After propensity score matching, the four groups demonstrated similar survival outcomes (3-year DFS: p = 0.533; 3-year OS: p = 0.328) and recurrence rates (10.3%, 12.1%, 10.3%, and 15.9% in the single-port, multi-port, and robot-assisted laparoscopy and laparotomy groups, respectively, p = 0.552). Recurrence most commonly occurred in distant organs. The single-port laparoscopy group had the longest operative time (205.1 ± 76.9 min) but the least blood loss (69.5 ± 90.8 mL) and the shortest postoperative hospital stay (5.2 ± 2.3 days). In contrast, the laparotomy group had the shortest operative time (163.4 ± 51.0 min) but the highest blood loss (368.3 ± 326.4 mL) and the longest postoperative hospital stay (10.3 ± 4.6 days). The transfusion rate was 0% in the single-port laparoscopy group and 3.7% in the laparotomy group. Notably, the laparotomy group had the highest wound complication rate (p = 0.001), whereas no wound hernias were observed in the three minimally invasive approaches. In conclusion, the survival outcomes were comparable between the methods, with the benefit of lower blood loss and shorter hospital stay observed in the single-port laparoscopy group. This study suggests that single-port laparoscopy is a feasible approach for endometrial cancer surgical staging.
Keywords: endometrial cancer; propensity score matching; single-port laparoscopy; staging surgery.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Comparison of Perioperative and Oncologic Outcomes with Laparotomy, and Laparoscopic or Robotic Surgery for Women with Endometrial Cancer.Asian Pac J Cancer Prev. 2015;16(13):5483-8. doi: 10.7314/apjcp.2015.16.13.5483. Asian Pac J Cancer Prev. 2015. PMID: 26225698
-
[Efficacy comparison between laparoscopy and open surgery in the treatment of gastric gastrointestinal stromal tumors larger than 2 cm using multicenter propensity score matching method].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Sep 25;23(9):888-895. doi: 10.3760/cma.j.cn.441530-20200616-00366. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 32927514 Chinese.
-
Initial experience with the da Vinci SP robot-assisted surgical staging of endometrial cancer: a retrospective comparison with conventional laparotomy.J Robot Surg. 2023 Dec;17(6):2889-2898. doi: 10.1007/s11701-023-01730-8. Epub 2023 Oct 10. J Robot Surg. 2023. PMID: 37816993
-
The Adoption of Single-port Laparoscopy for Full Staging of Endometrial Cancer: Surgical and Oncology Outcomes and Evaluation of the Learning Curve.J Minim Invasive Gynecol. 2017 Sep-Oct;24(6):1029-1036. doi: 10.1016/j.jmig.2017.06.017. Epub 2017 Jun 27. J Minim Invasive Gynecol. 2017. PMID: 28662990
-
Ultra-minimally invasive approaches for endometrial cancer treatment: review of the literature.Minerva Med. 2021 Feb;112(1):31-46. doi: 10.23736/S0026-4806.20.07073-1. Epub 2020 Nov 18. Minerva Med. 2021. PMID: 33205639
Cited by
-
Impact of a Surgical Approach on Endometrial Cancer Survival According to ESMO/ESGO Risk Classification: A Retrospective Multicenter Study in the Northern Italian Region.Cancers (Basel). 2025 Jul 7;17(13):2261. doi: 10.3390/cancers17132261. Cancers (Basel). 2025. PMID: 40647558 Free PMC article.
-
Surgical outcomes of single-port vs multi-port laparoscopic hysterectomy for endometrial cancer: A systematic review and meta-analysis.PLoS One. 2024 Dec 9;19(12):e0314997. doi: 10.1371/journal.pone.0314997. eCollection 2024. PLoS One. 2024. PMID: 39652553 Free PMC article.
References
-
- Colombo N., Creutzberg C., Amant F., Bosse T., González-Martín A., Ledermann J., Marth C., Nout R., Querleu D., Mirza M.R., et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016;27:16–41. doi: 10.1093/annonc/mdv484. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
